

doi: 10.1055/s-2008-1080995.
Transrectal ultrasound, manometry, and pudendal nerve terminal latency studies in the evaluation of sphincter injuries
Affiliations
- PMID: 20011414
- PMCID: PMC2780206
- DOI: 10.1055/s-2008-1080995
Item in Clipboard
Transrectal ultrasound, manometry, and pudendal nerve terminal latency studies in the evaluation of sphincter injuries
Clin Colon Rectal Surg.
2008 Aug.
Abstract
Fecal incontinence may be due to postpartum anal sphincter injuries or neurological damage even in the absence of obvious perineal trauma. Anal physiologic testing with transrectal ultrasound, manometry, and pudendal nerve terminal latency studies help to identify those patients with anal sphincter injuries who might benefit from anal sphincter repair. In this article, the authors discuss the specific tests that are available and how to interpret them.
Keywords: Anal sphincter injuries; anal physiology testing; fecal incontinence.
Figures
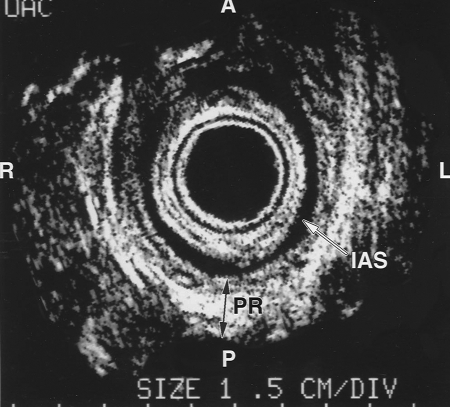
Normal anal ultrasound of the upper anal canal. The internal anal sphincter (IAS) is a darker band (white arrow) and the puborectalis (PR) is visualized as a white U-shaped structure (dark arrow) surrounding the IAS. The top of the figure is anterior. Reproduced with permission from the Cleveland Clinic Foundation, Cleveland, Ohio.
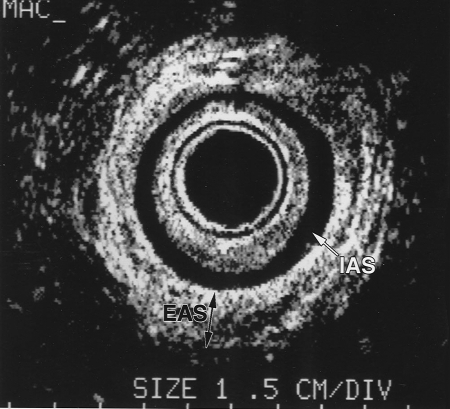
Normal anal ultrasound of the middle anal canal. The darker homogenous ring is the internal anal sphincter (IAS; white arrow). The white heterogeneous ring is the external anal sphincter (EAS; dark arrow). The external sphincter is forming a 360-degree intact circle. Reproduced with permission from the Cleveland Clinic Foundation, Cleveland, Ohio.
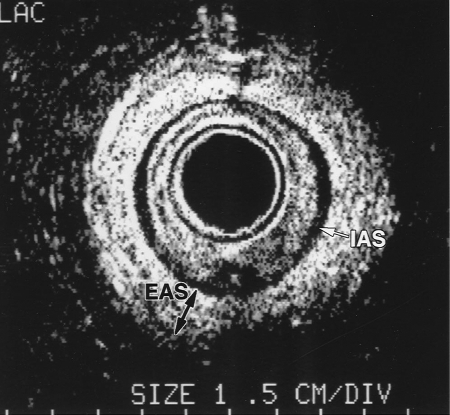
Normal anal ultrasound of the lower anal canal. The white heterogeneous ring represents the external anal sphincter (EAS), which is most prominent (dark arrow) at the lower anal canal. There is a thin darker rim of internal anal sphincter muscle (IAS; white arrow). Reproduced with permission from the Cleveland Clinic Foundation, Cleveland, Ohio.
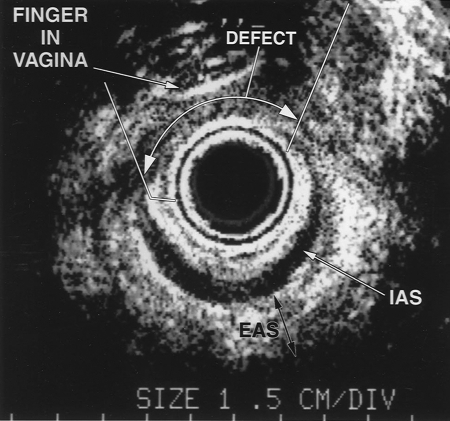
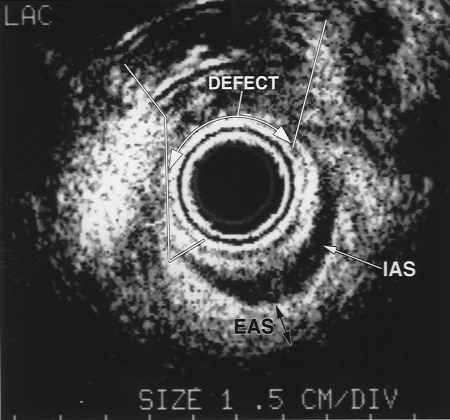
Transanal ultrasound image with a finger placed into the vagina and gentle application of pressure posteriorly. Discontinuity of the external anal sphincter and internal anal sphincter muscle is visualized (defect; white arrow). The darker inner ring is the internal anal sphincter (IAS; white arrow) and the darker outer ring is the external anal sphincter (EAS; dark arrow). Reproduced with permission from the Cleveland Clinic Foundation, Cleveland, Ohio.
Transanal ultrasound of traumatic anal sphincter injury. The large arrows represent the retracted muscle ends. Anteriorly there is disorganization and mixed echogenicity of the anterior defect. IAS, internal anal sphincter; EAS, external anal sphincter. Reproduced with permission from the Cleveland Clinic Foundation, Cleveland, Ohio.
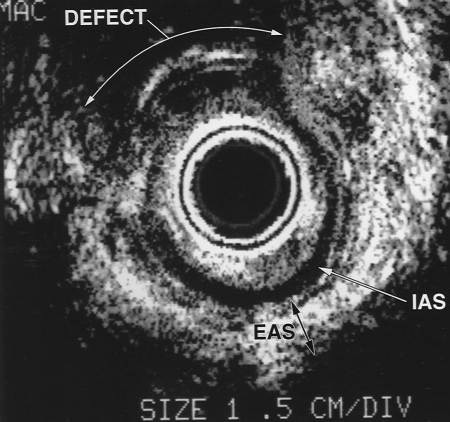
Transanal ultrasound of traumatic anal sphincter injury. The large arrows represent the retracted muscle ends. Anteriorly there is disorganization and mixed echogenicity of the anterior defect. IAS, internal anal sphincter; EAS, external anal sphincter. Reproduced with permission from the Cleveland Clinic Foundation, Cleveland, Ohio.

B-K Medical (Herlev, Denmark) three-dimensional (3D) anorectal ultrasound equipment. The data from a series of closely spaced two dimensional images is combined to create a 3D image that can be freely rotated and sliced. The data stored in a file originating from one acquisition can be reviewed many times. Reproduced with permission from the Cleveland Clinic Foundation, Cleveland, Ohio.

B-K Medical (Herlev, Denmark) ultrasound three-dimensional (3D) probe type 2050. There is a built in high resolution 3D acquisition system that can be operated at different levels of definition. Reproduced with permission from the Cleveland Clinic Foundation, Cleveland, Ohio.
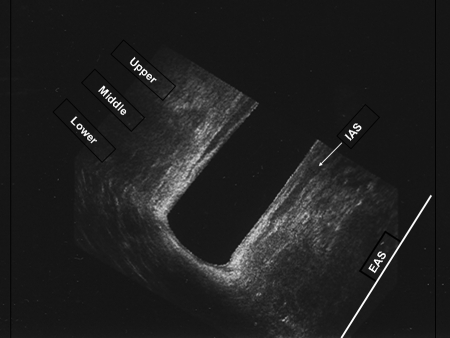
Transanal ultrasound three-dimensional (3D) coronal view of normal anal canal. The upper, middle, and lower anal canals are depicted. The darker interior is the internal sphincter muscle (IAS; white arrow) and the whiter tissue is the external sphincter muscle. Reproduced with permission from the Cleveland Clinic Foundation, Cleveland, Ohio.
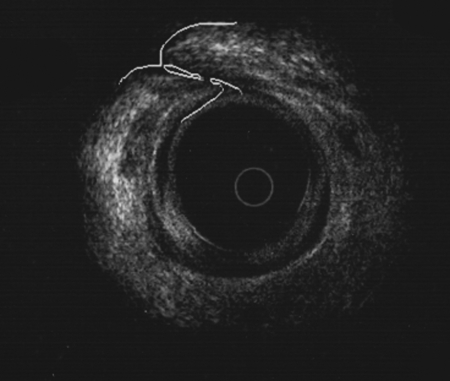
Transanal ultrasound of overlapping sphincter repair. The white outer circle represents the external anal sphincter complex, which is overlapped after sphincter repair. Reproduced with permission from the Cleveland Clinic Foundation, Cleveland, Ohio.
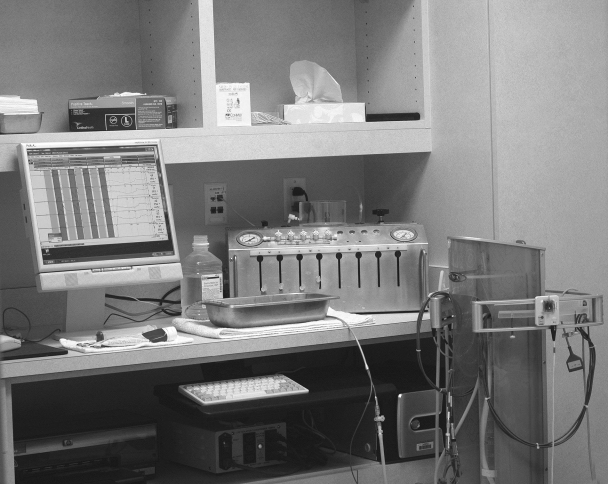
Anal manometry apparatus. The electronic catheter (Triton; Laborie Corp., Toronto, Canada) is linked to the polygraph and computer monitor. Reproduced with permission from the Cleveland Clinic Foundation, Cleveland, Ohio.
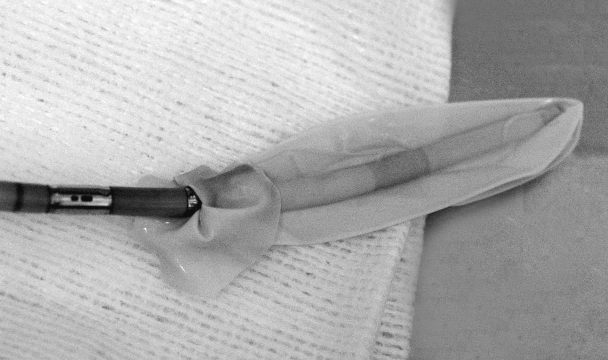
Manometry catheter with balloon. This is an electronic manometry catheter (Unisensor USA, New York, NY) with four sensors. A balloon is tied to the end of the catheter for evaluation of rectal sensation. Reproduced with permission from the Cleveland Clinic Foundation, Cleveland, Ohio.
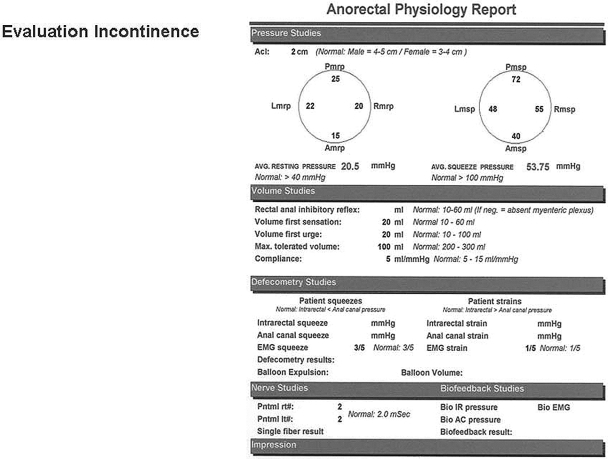
Anal physiology report. Normal values identified for this laboratory are reported after each of the measurements. Reproduced with permission from the Cleveland Clinic Foundation, Cleveland, Ohio.

Pudendal nerve stimulating electrode (Dantec, Skovlunde, Denmark) mounted on the examiners gloved finger. Reproduced with permission from the Cleveland Clinic Foundation, Cleveland, Ohio.
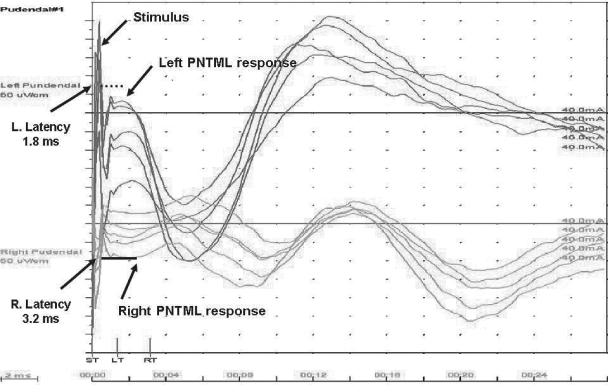
Pudendal nerve terminal latency tracing. The left and right tracings are superimposed on one another. The stimulus is the large spike and muscular response is visualized at the take off of the curve (arrows). The latency measurement is the difference of the stimulus to the muscular contraction (arrows). On the left, the measurement is normal at 1.8 milliseconds. On the right, it is delayed at 3.2 milliseconds. Normal values are 2.0 ± 2 milliseconds.
Similar articles
-
Delayed pudendal nerve conduction and endosonographic appearance of the anal sphincter complex.Dis Colon Rectum. 2000 Dec;43(12):1689-94. doi: 10.1007/BF02236851. Dis Colon Rectum. 2000. PMID: 11156452
-
Pudendal nerve damage increases the risk of fecal incontinence in women with anal sphincter rupture after childbirth.Acta Obstet Gynecol Scand. 1995 Jul;74(6):434-40. doi: 10.3109/00016349509024405. Acta Obstet Gynecol Scand. 1995. PMID: 7604686 Clinical Trial.
-
The utility of pudendal nerve terminal motor latencies in idiopathic incontinence.Dis Colon Rectum. 2006 Jun;49(6):852-7. doi: 10.1007/s10350-006-0529-y. Dis Colon Rectum. 2006. PMID: 16598403
-
Fecal incontinence. Studies on physiology, pathophysiology and surgical treatment.Dan Med Bull. 2003 Aug;50(3):262-82. Dan Med Bull. 2003. PMID: 13677243 Review.
-
[Postpartum fecal incontinence. State of the problem].Khirurgiia (Mosk). 2022;(6):127-132. doi: 10.17116/hirurgia2022061127. Khirurgiia (Mosk). 2022. PMID: 35658144 Review. Russian.
Cited by
-
Establishing a peripartum perineal trauma clinic: a narrative review.Int Urogynecol J. 2021 Jul;32(7):1653-1662. doi: 10.1007/s00192-020-04631-8. Epub 2021 Jan 5. Int Urogynecol J. 2021. PMID: 33399903 Review.
-
Anal Sphincter Defect and Fecal Incontinence.JPGN Rep. 2022 Oct 20;3(4):e254. doi: 10.1097/PG9.0000000000000254. eCollection 2022 Nov. JPGN Rep. 2022. PMID: 37168467 Free PMC article.
-
Advances in motility testing--current and novel approaches.Nat Rev Gastroenterol Hepatol. 2013 Aug;10(8):463-72. doi: 10.1038/nrgastro.2013.80. Epub 2013 May 7. Nat Rev Gastroenterol Hepatol. 2013. PMID: 23648939 Review.
-
Dynamic transperineal ultrasonography correlates with prolonged pudendal nerve latency in female with fecal incontinence.Updates Surg. 2020 Dec;72(4):1187-1194. doi: 10.1007/s13304-020-00838-y. Epub 2020 Jun 28. Updates Surg. 2020. PMID: 32596803
-
An Evidence-Based Approach to the Evaluation, Diagnostic Assessment and Treatment of Fecal Incontinence in Women.Curr Obstet Gynecol Rep. 2014 Sep;3(3):155-164. doi: 10.1007/s13669-014-0085-8. Curr Obstet Gynecol Rep. 2014. PMID: 25505643 Free PMC article.
References
-
- Johanson J F, Lafferty J. Epidemiology of fecal incontinence: the silent affliction. Am J Gastroenterol. 1996;91:33–36. - PubMed
-
- Sultan A H, Kamm M A, Hudson C N, et al. Anal sphincter disruption during vaginal delivery. N Engl J Med. 1993;329:1956–1957. - PubMed
-
- Donnelly V, O'Connell P R, O'Herlihy C. The influence of oestrogen replacement on faecal incontinence in post menopausal women. Br J Obstet Gynaecol. 1997;104:311–315. - PubMed
-
- Nichols C M, Ramakrishnan V, Gill E J, Hurt W G. Anal incontinence in women with and those without pelvic floor disorders. Obstet Gynecol. 2005;106(6):1266–1271. - PubMed
-
- Willis S, Faridi A, Schelzig S, et al. Childbirth and incontinence: a prospective study on anal sphincter morphology and function before and early after vaginal delivery. Arch Surg. 2002;387:101–107. - PubMed
