

Computed tomography enterography and magnetic resonance enterography: the future of small bowel imaging
- PMID: 20011418
- PMCID: PMC2780209
- DOI: 10.1055/s-2008-1080999
Computed tomography enterography and magnetic resonance enterography: the future of small bowel imaging
Abstract
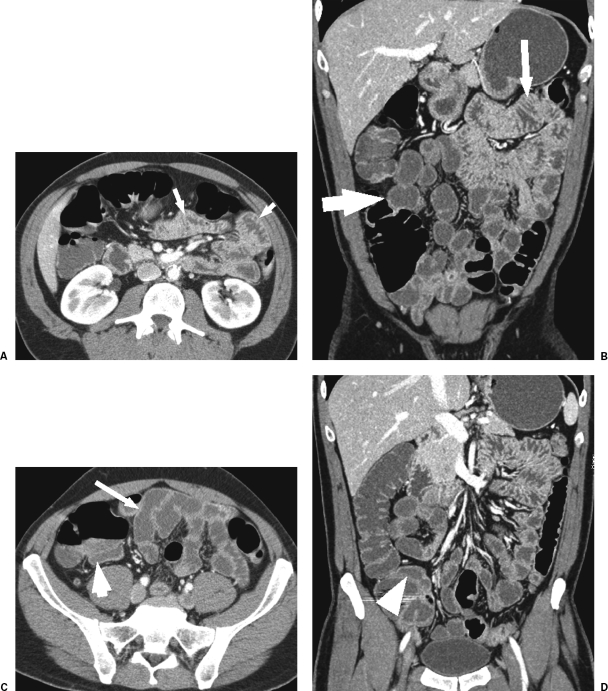
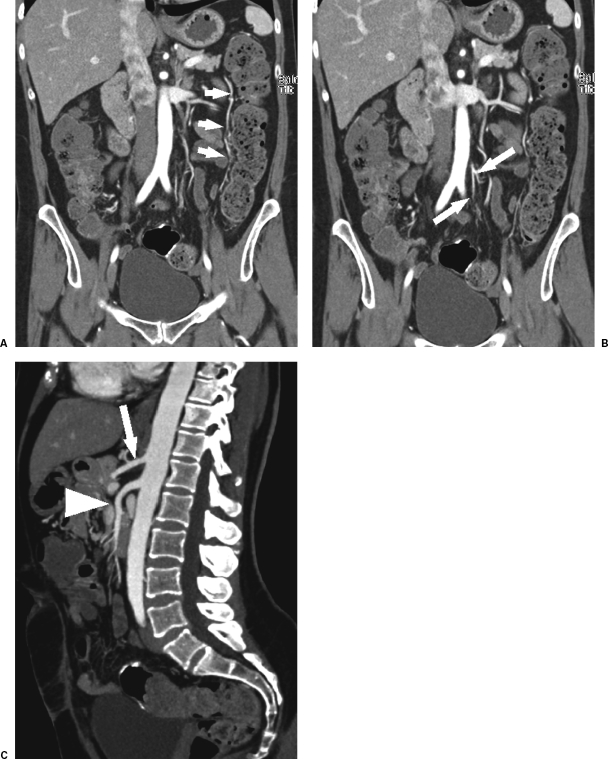
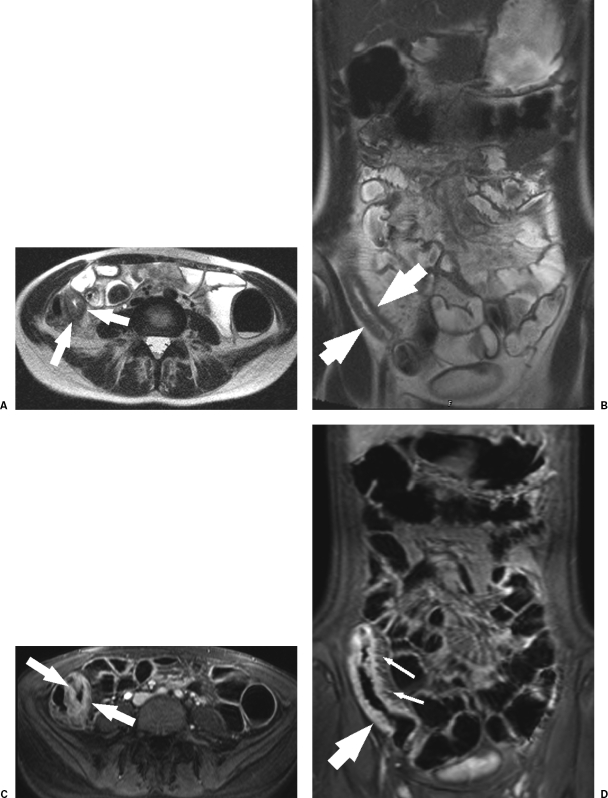
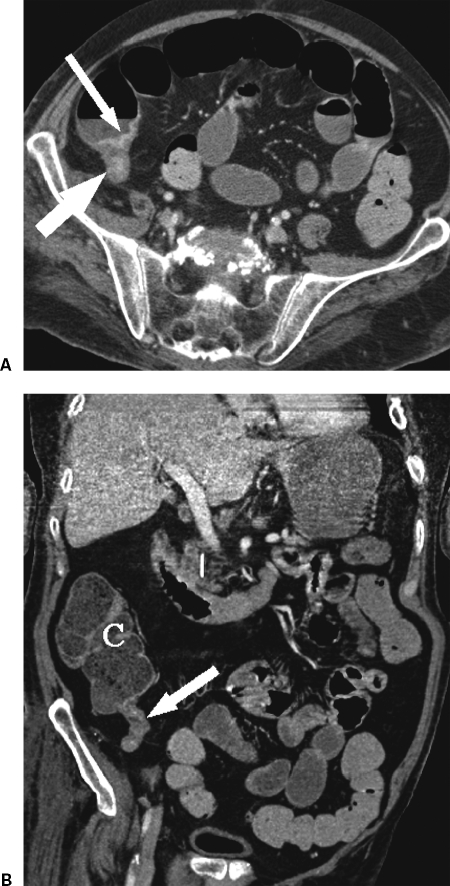
In the last 5 years, computed tomography enterography (CTE) and to a lesser extent magnetic resonance enterography (MRE) have supplanted the routine small bowel series and enteroclysis in the evaluation of many small bowel diseases, especially Crohn's disease. Both CTE and MRE use similar methods of bowel lumen opacification and distension and both have distinct advantages and disadvantages. Both have been most extensively studied in patients with Crohn's disease. What is certain is that these cross-sectional examinations have largely replaced the historic fluoroscopic examinations in the evaluation of the small bowel.
Keywords: Computed tomography enterography; Crohn's disease; chronic obscure gastrointestinal bleeding; magnetic resonance enterography.
Figures

References
-
- Prokop M. Multislice CT: technical principles and future trends. Eur Radiol. 2003;13(Suppl 5):M3–M13. - PubMed
-
- Horton K M, Fishman E K. Volume-rendered 3D CT of the mesenteric vasculature: normal anatomy, anatomic variants, and pathologic conditions. Radiographics. 2002;22(1):161–172. - PubMed
-
- Horton K M, Fishman E K. The current status of multidetector row CT and three-dimensional imaging of the small bowel. Radiol Clin North Am. 2003;41(2):199–212. - PubMed
-
- Raptopoulos V, Davis M A, Davidoff A, et al. Fat-density oral contrast agent for abdominal CT. Radiology. 1987;164(3):653–656. - PubMed
-
- Angelelli G, Macarini L, Fratello A. Use of water as an oral contrast agent for CT study of the stomach. AJR Am J Roentgenol. 1987;149(5):1084. [letter] - PubMed
