

Management of the malignant polyp
- PMID: 20011440
- PMCID: PMC2780260
- DOI: 10.1055/s-0028-1089944
Management of the malignant polyp
Abstract
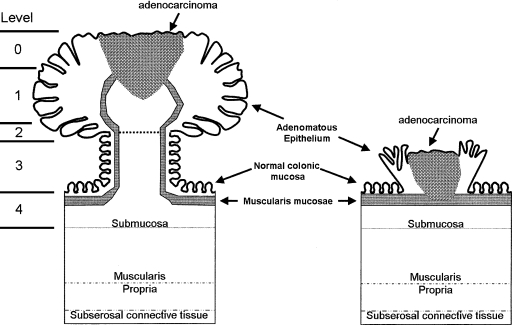
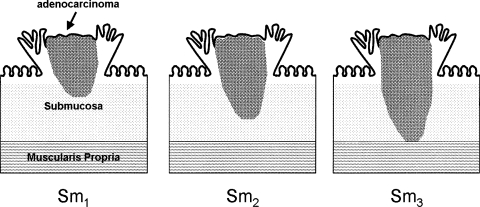
In the United States, the prevalence of adenomatous polyps found during colonoscopic evaluation ranges from 25 to 41%, and of these, 2 to 5% contain invasive malignancy. The management of the malignant polyp continues to be challenging. Endoscopic resection by polypectomy has been shown to be sufficient for management of certain polyps containing cancer; however, it is important to keep in mind that polypectomy does not remove the lymph node drainage basin and may be an inadequate resection for some adenocarcinoma containing polyps that have specific histologic features. Depth of invasion has been shown to correlate with the risk of lymph node metastasis. Other unfavorable histologic features include lymphovascular invasion, poor differentiation, inability to assess margin (piecemeal resection), and positive resection margin (< 2 mm); these are important factors to consider in management. For these patients formal oncologic surgical resection is indicated. Traditional open or laparoscopic procedures are routinely used for colectomy in these patients. Following polypectomy or segmental colectomy, surveillance of these patients is critical, and can lead to excellent long-term outcomes.
Keywords: Haggitt level; Malignant polyp; adenocarcinoma; adenomatous polyp; endoscopic polypectomy; segmental colectomy.
Figures
Similar articles
-
Rate of residual disease after complete endoscopic resection of malignant colonic polyp.Dis Colon Rectum. 2012 Feb;55(2):122-7. doi: 10.1097/DCR.0b013e3182336c38. Dis Colon Rectum. 2012. PMID: 22228153
-
Adverse Histologic Features in Colorectal Nonpedunculated Malignant Polyps With Nodal Metastasis.Am J Surg Pathol. 2020 Feb;44(2):241-246. doi: 10.1097/PAS.0000000000001369. Am J Surg Pathol. 2020. PMID: 31498179
-
Malignant colon polyps--cure by colonoscopy or colectomy?Am J Gastroenterol. 1984 Jul;79(7):543-7. Am J Gastroenterol. 1984. PMID: 6741907
-
Polypectomy or colectomy? Management of 106 consecutively encountered colorectal polyps.Am Surg. 1988 Feb;54(2):93-9. Am Surg. 1988. PMID: 3277505 Review.
-
Combined Endoscopic Laparoscopic Surgery Procedures for Colorectal Surgery.Clin Colon Rectal Surg. 2017 Apr;30(2):145-150. doi: 10.1055/s-0036-1597321. Clin Colon Rectal Surg. 2017. PMID: 28381946 Free PMC article. Review.
Cited by
-
Colorectal carcinoma: Pathologic aspects.J Gastrointest Oncol. 2012 Sep;3(3):153-73. doi: 10.3978/j.issn.2078-6891.2012.030. J Gastrointest Oncol. 2012. PMID: 22943008 Free PMC article.
-
Management of malignant colon polyps: current status and controversies.World J Gastroenterol. 2014 Nov 21;20(43):16178-83. doi: 10.3748/wjg.v20.i43.16178. World J Gastroenterol. 2014. PMID: 25473171 Free PMC article. Review.
-
Ileocecal Valve Sparing Resection for the Treatment of Benign Cecal Polyps Unsuitable for Polypectomy.JSLS. 2021 Apr-Jun;25(2):e2021.00023. doi: 10.4293/JSLS.2021.00023. JSLS. 2021. PMID: 34316245 Free PMC article.
-
Complex rectal polyps: other treatment modalities required when offering a transanal endoscopic microsurgery service.Int J Colorectal Dis. 2011 Sep;26(9):1177-82. doi: 10.1007/s00384-011-1212-x. Epub 2011 May 7. Int J Colorectal Dis. 2011. PMID: 21553009
-
Prediction of Lymph Node Metastasis in T1 Colorectal Cancer Using Artificial Intelligence with Hematoxylin and Eosin-Stained Whole-Slide-Images of Endoscopic and Surgical Resection Specimens.Cancers (Basel). 2024 May 16;16(10):1900. doi: 10.3390/cancers16101900. Cancers (Basel). 2024. PMID: 38791978 Free PMC article.
References
-
- National Cancer Institute Types of colon and rectal cancer. Available at: http://www.cancer.gov/cancertopics/types/colon-and -rectal. Accessed September 16, 2008. Available at: http://www.cancer.gov/cancertopics/types/colon-and -rectal
-
- Markowitz A J, Winawer S J. Management of colorectal polyps. CA Cancer J Clin. 1997;47(2):93–112. - PubMed
-
- Winawer S J, Zauber A G, O'Brien M D, et al. The National Polyp Study: design, methods, and characteristics of patients with newly diagnosed polyps. Cancer. 1992;70:1236–1245. - PubMed
-
- Rex D K, Lehman G A, Hawes R H, Ulbright T M, Smith J J. Screening colonoscopy in asymptomatic average risk persons with negative fecal occult blood tests. Gastroenterology. 1991;100:64–67. - PubMed
-
- Lieberman D A, Smith F W. Screening for colon malignancy with colonoscopy. Am J Gastroenterol. 1991;86:946–951. - PubMed
