

IFNgamma response to Mycobacterium tuberculosis, risk of infection and disease in household contacts of tuberculosis patients in Colombia
- PMID: 20011589
- PMCID: PMC2788133
- DOI: 10.1371/journal.pone.0008257
IFNgamma response to Mycobacterium tuberculosis, risk of infection and disease in household contacts of tuberculosis patients in Colombia
Abstract
Objectives: Household contacts (HHCs) of pulmonary tuberculosis patients are at high risk of Mycobacterium tuberculosis infection and early disease development. Identification of individuals at risk of tuberculosis disease is a desirable goal for tuberculosis control. Interferon-gamma release assays (IGRAs) using specific M. tuberculosis antigens provide an alternative to tuberculin skin testing (TST) for infection detection. Additionally, the levels of IFNgamma produced in response to these antigens may have prognostic value. We estimated the prevalence of M. tuberculosis infection by IGRA and TST in HHCs and their source population (SP), and assessed whether IFNgamma levels in HHCs correlate with tuberculosis development.
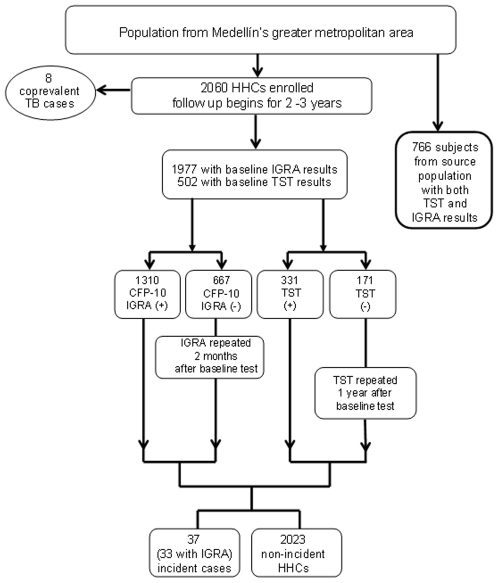
Methods: A cohort of 2060 HHCs was followed for 2-3 years after exposure to a tuberculosis case. Besides TST, IFNgamma responses to mycobacterial antigens: CFP, CFP-10, HspX and Ag85A were assessed in 7-days whole blood cultures and compared to 766 individuals from the SP in Medellín, Colombia. Isoniazid prophylaxis was not offered to child contacts because Colombian tuberculosis regulations consider it only in children under 5 years, TST positive without BCG vaccination.
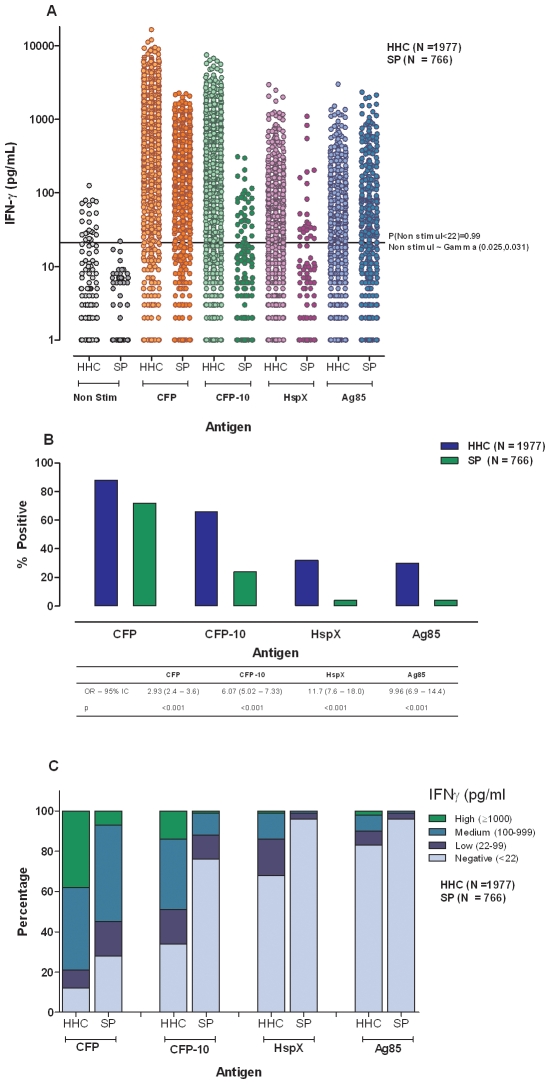
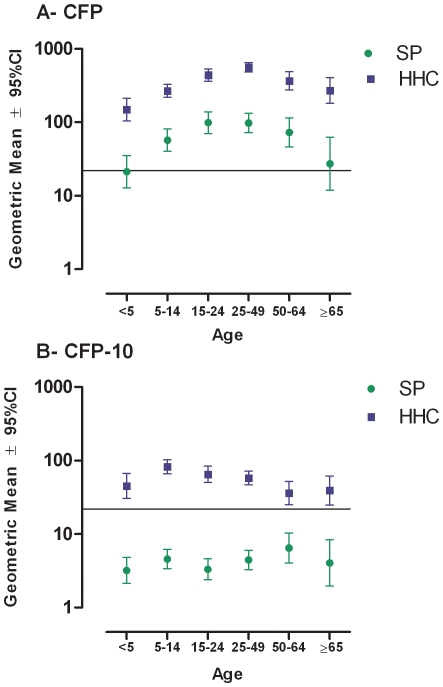
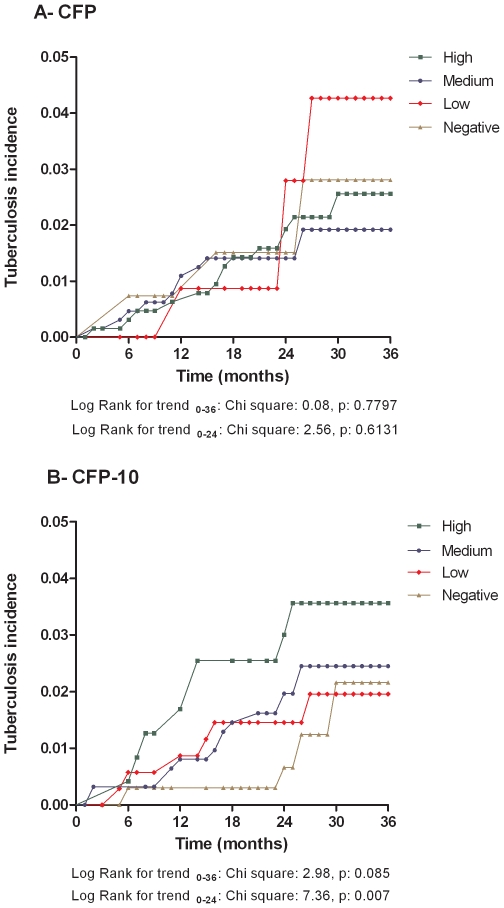
Results: Using TST 65.9% of HHCs and 42.7% subjects from the SP were positive (OR 2.60, p<0.0001). IFNgamma response to CFP-10, a biomarker of M. tuberculosis infection, tested positive in 66.3% HHCs and 24.3% from the SP (OR = 6.07, p<0.0001). Tuberculosis incidence rate was 7.0/1000 person years. Children <5 years accounted for 21.6% of incident cases. No significant difference was found between positive and negative IFNgamma responders to CFP-10 (HR 1.82 95% CI 0.79-4.20 p = 0.16). However, a significant trend for tuberculosis development amongst high HHC IFNgamma producers was observed (trend Log rank p = 0.007).
Discussion: CFP-10-induced IFNgamma production is useful to establish tuberculosis infection prevalence amongst HHC and identify those at highest risk of disease. The high tuberculosis incidence amongst children supports administration of chemoprophylaxis to child contacts regardless of BCG vaccination.
Conflict of interest statement
Figures
Similar articles
-
Broad adaptive immune responses to M. tuberculosis antigens precede TST conversion in tuberculosis exposed household contacts in a TB-endemic setting.PLoS One. 2014 Dec 30;9(12):e116268. doi: 10.1371/journal.pone.0116268. eCollection 2014. PLoS One. 2014. PMID: 25549338 Free PMC article.
-
Prevalence of latent tuberculosis infection in Sudan: a case-control study comparing interferon-γ release assay and tuberculin skin test.BMC Public Health. 2013 Dec 5;13:1128. doi: 10.1186/1471-2458-13-1128. BMC Public Health. 2013. PMID: 24313987 Free PMC article.
-
Immune correlates of acute Mycobacterium tuberculosis infection in household contacts in Kampala, Uganda.Am J Trop Med Hyg. 2006 Jul;75(1):55-61. Am J Trop Med Hyg. 2006. PMID: 16837709 Free PMC article.
-
[Evolution of IGRA researches].Kekkaku. 2008 Sep;83(9):641-52. Kekkaku. 2008. PMID: 18979999 Review. Japanese.
-
Interferon gamma release assays: principles and practice.Enferm Infecc Microbiol Clin. 2010 Apr;28(4):245-52. doi: 10.1016/j.eimc.2009.05.012. Epub 2009 Sep 24. Enferm Infecc Microbiol Clin. 2010. PMID: 19783328 Review.
Cited by
-
Diagnosing latent tuberculosis in high-risk individuals: rising to the challenge in high-burden areas.J Infect Dis. 2011 Nov 15;204 Suppl 4(Suppl 4):S1168-78. doi: 10.1093/infdis/jir449. J Infect Dis. 2011. PMID: 21996699 Free PMC article. Review.
-
Immunodiagnosis of tuberculosis: a dynamic view of biomarker discovery.Clin Microbiol Rev. 2011 Oct;24(4):792-805. doi: 10.1128/CMR.00014-11. Clin Microbiol Rev. 2011. PMID: 21976609 Free PMC article. Review.
-
Predictive value of TNF-α, IFN-γ, and IL-10 for tuberculosis among recently exposed contacts in the United States and Canada.BMC Infect Dis. 2020 Jul 31;20(1):553. doi: 10.1186/s12879-020-05185-2. BMC Infect Dis. 2020. PMID: 32736606 Free PMC article.
-
Risk of infection and disease progression in children exposed to tuberculosis at home, Colombia.Colomb Med (Cali). 2019 Dec 30;50(4):261-274. doi: 10.25100/cm.v50i4.4185. Colomb Med (Cali). 2019. PMID: 32476692 Free PMC article.
-
Predictive value of interferon-γ release assays for incident active tuberculosis: a systematic review and meta-analysis.Lancet Infect Dis. 2012 Jan;12(1):45-55. doi: 10.1016/S1473-3099(11)70210-9. Epub 2011 Aug 16. Lancet Infect Dis. 2012. PMID: 21846592 Free PMC article.
References
-
- World Health Organization. Global Tuberculosis Control:Surveillance, Planning, Financing:WHO Report 2008. Geneva, Switzerland: WHO; 2008.
-
- Morrison J, Pai M, Hopewell PC. Tuberculosis and latent tuberculosis infection in close contacts of people with pulmonary tuberculosis in low-income and middle-income countries: a systematic review and meta-analysis. Lancet Infect Dis. 2008;8:359–368. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
