

IgG autoantibody to brain beta tubulin III associated with cytokine cluster-II discriminate cerebral malaria in central India
- PMID: 20011600
- PMCID: PMC2788233
- DOI: 10.1371/journal.pone.0008245
IgG autoantibody to brain beta tubulin III associated with cytokine cluster-II discriminate cerebral malaria in central India
Abstract
Background: The main processes in the pathogenesis of cerebral malaria caused by Plasmodium falciparum involved sequestration of parasitized red blood cells and immunopathological responses. Among immune factors, IgG autoantibodies to brain antigens are increased in P. falciparum infected patients and correlate with disease severity in African children. Nevertheless, their role in the pathophysiology of cerebral malaria (CM) is not fully defined. We extended our analysis to an Indian population with genetic backgrounds and endemic and environmental status different from Africa to determine if these autoantibodies could be either a biomarker or a risk factor of developing CM.
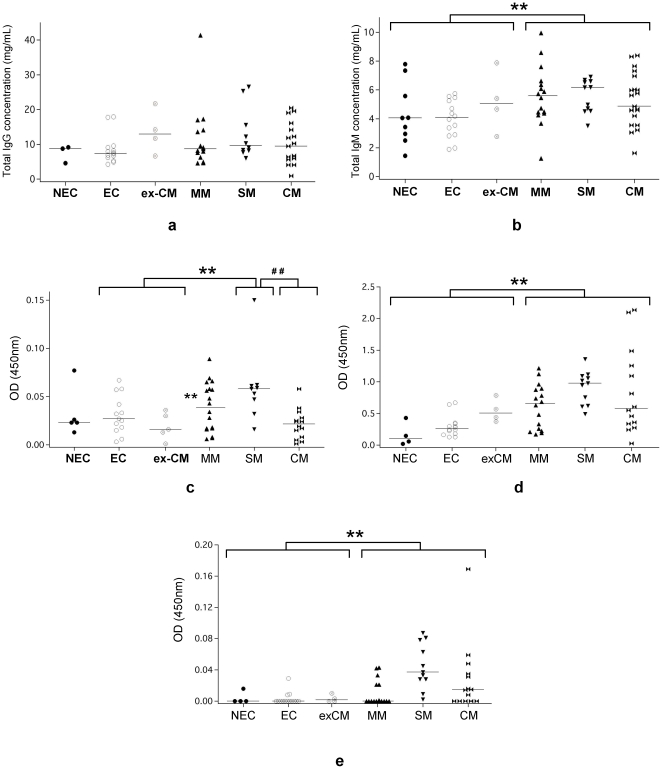
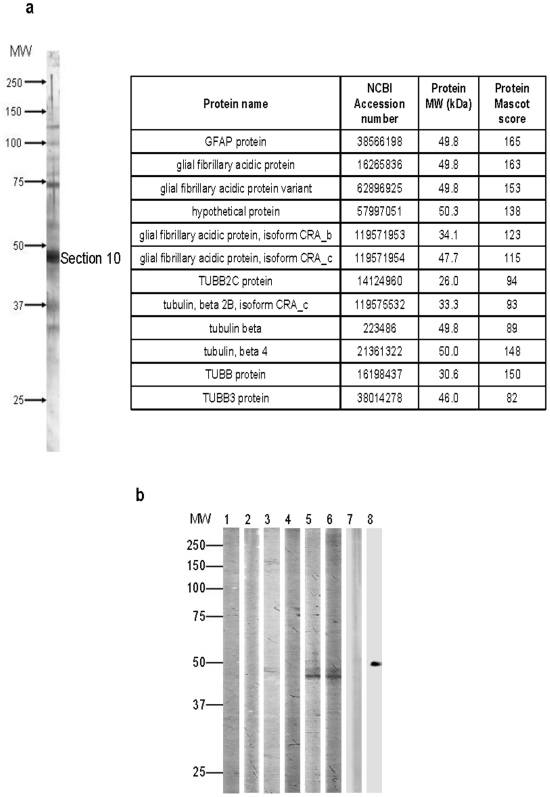
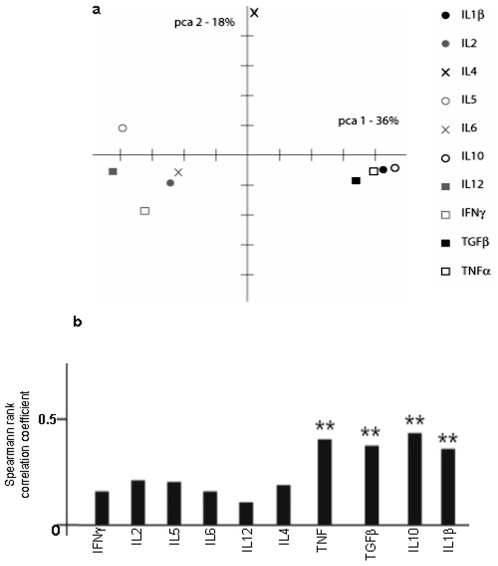
Methods/principal findings: We investigated the significance of these self-reactive antibodies in clinically well-defined groups of P. falciparum infected patients manifesting mild malaria (MM), severe non-cerebral malaria (SM), or cerebral malaria (CM) and in control subjects from Gondia, a malaria epidemic site in central India using quantitative immunoprinting and multivariate statistical analyses. A two-fold complete-linkage hierarchical clustering allows classifying the different patient groups and to distinguish the CM from the others on the basis of their profile of IgG reactivity to brain proteins defined by PANAMA Blot. We identified beta tubulin III (TBB3) as a novel discriminant brain antigen in the prevalence of CM. In addition, circulating IgG from CM patients highly react with recombinant TBB3. Overall, correspondence analyses based on singular value decomposition show a strong correlation between IgG anti-TBB3 and elevated concentration of cluster-II cytokine (IFNgamma, IL1beta, TNFalpha, TGFbeta) previously demonstrated to be a predictor of CM in the same population.
Conclusions/significance: Collectively, these findings validate the relationship between antibody response to brain induced by P. falciparum infection and plasma cytokine patterns with clinical outcome of malaria. They also provide significant insight into the immune mechanisms associated to CM by the identification of TBB3 as a new disease-specific marker and potential therapeutic target.
Conflict of interest statement
Figures





References
-
- Korenromp E. World Malaria Report: Roll Back Malaria. World Health Organization: Geneva 2004
-
- Breman JG, Egan A, Keusch GT. The intolerable burden of malaria: a new look at the numbers. Am J Trop Med Hyg. 2001;64:iv–vii. - PubMed
-
- Mazier D, Nitcheu J, Idrissa-Boubou M. Cerebral malaria and immunogentics. Parasite Immunol. 2000;22:613–23. - PubMed
-
- Miller LH, Baruch DI, Marsh K, Doumbo OK. The pathogenic basis of malaria. Nature. 2002;415:673–9. - PubMed
-
- Greenwood BM. The epidemiology of malaria. Ann Trop Med Parasitol. 1997;91:763–9. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
