

Nonunions around the knee joint
- PMID: 20012745
- PMCID: PMC2899352
- DOI: 10.1007/s00264-009-0924-9
Nonunions around the knee joint
Abstract
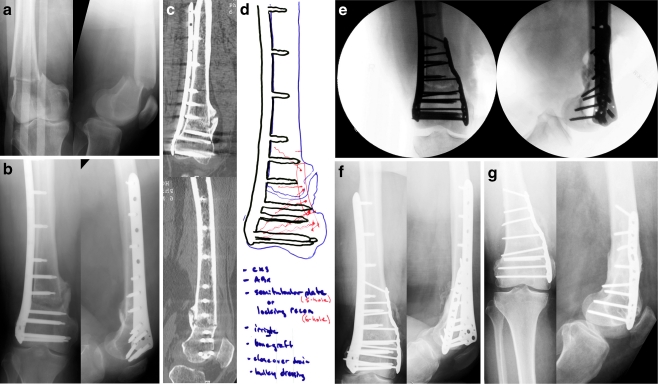
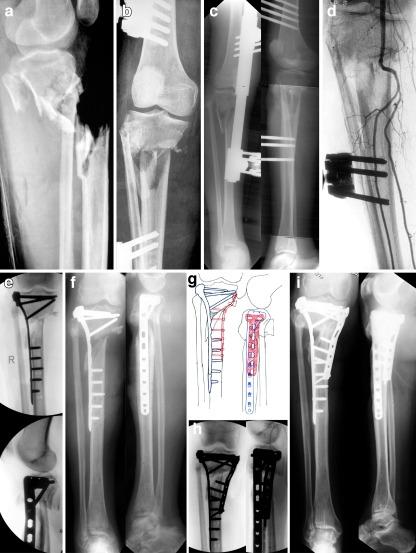
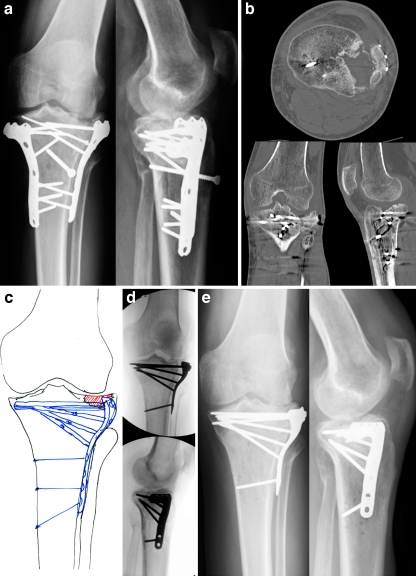
Nonunions of the distal femur are relatively rare but can occur with or without previous surgery. Many surgical methods have been described for the treatment of these nonunions including external fixation, intramedullary nailing, arthroplasty, and fixed angle plating. While arthroplasty may have a limited role in the elderly patient with osteoporosis and severe communiution, most nonunions can be reliably treated with revision fixation using a fixed angled device, lag screws, and bone grafting as needed. Fixed-angle plating also has the advantage of stabilising a small distal segment where intramedullary nailing has proven to be less effective. Any surgical intervention must include restoration of the normal mechanical axis of the distal femur for a satisfactory clinical outcome. Proximal tibia nonunions are a similarly rare clinical entity due to the excellent blood supply in the metaphysis. Extra-articular proximal tibial nonunions are often due to malreduction during the index surgery resulting in poor bone contact and biomechanical stability. Soft tissue forces and improper use of intramedullary implants often predispose these fractures to malalignment. Revision surgery consisting of deformity correction and at least a lateral tension band plate with lag screws has led to predictable union and good clinical results. Tibial plateau nonunions are exceedingly uncommon but are difficult to treat because of small, often devascularised fragments, post-surgical scarring, and osteopenia. Revision surgery with meticulous soft tissue handling to restore the articular surface and mechanical axis with repair of meniscal pathology gives the patient the best chance of recovering knee function.
Figures
References
-
- Altenberg AR, Shorkey RL. Blade-plate fixation in non-union and in complicated fractures of the supracondylar region of the femur. J Bone Jt Surg. 1949;31A(2):312–316. - PubMed
-
- Connolly JF, Dehne E. Closed reduction and early cast-brace ambulation in the treatment of femoral fractures. J Bone Jt Surg. 1973;55-A:1581–1599. - PubMed
-
- Weil GC, Kuehner HG, Henry JP. The treatment of 278 consecutive fractures of the femur. Surg Gynecol Obstet. 1936;62(435):441.
-
- Danziger MB, Caucei D, Zecher SB, Segal D, Covall DJ. Treatment of intercondylar and supracondylar distal femoral fractures using the GSH supracondylar nail. Am J Orthop. 1995;24(9):684–690. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
