

The growth hormone receptor (GHR) polymorphism in growth-retarded children with Cushing disease: lack of association with growth and measures of the somatotropic axis
- PMID: 20013551
- PMCID: PMC3412355
- DOI: 10.1055/s-0029-1242744
The growth hormone receptor (GHR) polymorphism in growth-retarded children with Cushing disease: lack of association with growth and measures of the somatotropic axis
Abstract
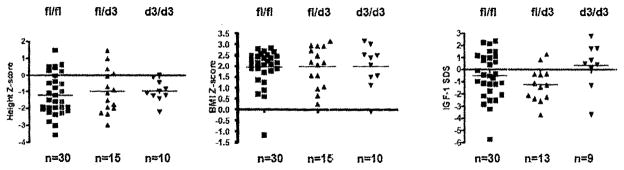
Pediatric Cushing disease (CD) often presents with short stature, but we have observed significant inter-individual variability in the growth delay caused by endogenous hypercortisolism. Glucocorticoids cause growth retardation by affecting the growth hormone (GH) - insulin-like growth factor-1 (IGF 1) somatotropic axis, but also other, GH-independent sites. Recently, the GH receptor (GHR) gene was found to have a common polymorphism (P) that leads to a deletion (d3) or retention of exon 3. In this study, we tested the hypothesis that the GH receptor polymorphism (GHR-P) maybe one of the significant variants that determines the degree of growth delay among patients with CD. GHR genotyping was performed on 56 children with newly diagnosed CD (24 females, 32 males, mean age of 12.9+/-3.3 years) who were followed at our institution between the years 1997-2007. Correlation analysis included genotype, measures of growth and the somatotropic axis, and anthropometrics. Within the group, 31 (12 girls, 19 boys) expressed the full length GHR allele, 10 (4 girls, 6 boys) were d3-GHR homozygotes and 15 (7 girls, 8 boys) were d3-GHR heterozygotes. No significant differences were found between the GHR genotypes and patient's height and/or growth velocity, or any other measures that we evaluated. The presence of a well-studied and common GHR polymorphism does not appear to be responsible for the variability of growth delay observed in patients with Cushing disease.
Figures
Similar articles
-
The d3-growth hormone (GH) receptor polymorphism is associated with increased responsiveness to GH in Turner syndrome and short small-for-gestational-age children.J Clin Endocrinol Metab. 2006 Feb;91(2):659-64. doi: 10.1210/jc.2005-1581. Epub 2005 Nov 15. J Clin Endocrinol Metab. 2006. PMID: 16291706
-
The exon 3-deleted/full-length growth hormone receptor polymorphism and response to growth hormone therapy in growth hormone deficiency and Turner syndrome: a multicenter study.Horm Res Paediatr. 2012;77(2):85-93. doi: 10.1159/000335172. Epub 2012 Mar 23. Horm Res Paediatr. 2012. PMID: 22456308
-
The exon 3-deleted/full-length growth hormone receptor polymorphism did not influence growth response to growth hormone therapy over two years in prepubertal short children born at term with adequate weight and length for gestational age.J Clin Endocrinol Metab. 2008 Mar;93(3):764-70. doi: 10.1210/jc.2007-2180. Epub 2007 Dec 26. J Clin Endocrinol Metab. 2008. PMID: 18160465
-
The exon 3-deleted growth hormone receptor: molecular and functional characterization and impact on GH/IGF-I axis in physiological and pathological conditions.J Endocrinol Invest. 2011 Dec;34(11):861-8. doi: 10.1007/BF03346731. J Endocrinol Invest. 2011. PMID: 22322534 Review.
-
MECHANISMS IN ENDOCRINOLOGY: Clinical and pharmacogenetic aspects of the growth hormone receptor polymorphism.Eur J Endocrinol. 2017 Dec;177(6):R309-R321. doi: 10.1530/EJE-17-0549. Epub 2017 Sep 13. Eur J Endocrinol. 2017. PMID: 28904008 Review.
References
-
- Savage MO, Storr HL, Grossman AB, Krassas GE. Growth and growth hormone secretion in paediatric Cushing’s disease. Hormones (Athens, Greece) 2003;2:93–97. - PubMed
-
- Voutilainen R, Leisti S, Perheentupa J. Growth in Cushing syndrome. Eur J Pediatr. 1985;144:141–145. - PubMed
-
- Storr HL, Chan LF, Grossman AB, Savage MO. Paediatric Cushing’s syndrome: epidemiology, investigation and therapeutic advances. Trends Endocrinol Metab: TEM. 2007;18:167–174. - PubMed
-
- Hochberg Z. Mechanisms of steroid impairment of growth. Horm Res. 2002;58 (Suppl 1):33–38. - PubMed
-
- Magiakou MA, Mastorakos G, Gomez MT, Rose SR, Chrousos GP. Suppressed spontaneous and stimulated growth hormone secretion in patients with Cushing’s disease before and after surgical cure. J Clin Endocrinol Metab. 1994;78:131–137. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
