

Immunological and clinical profile of adult patients with selective immunoglobulin subclass deficiency: response to intravenous immunoglobulin therapy
- PMID: 20015274
- PMCID: PMC2819500
- DOI: 10.1111/j.1365-2249.2009.04062.x
Immunological and clinical profile of adult patients with selective immunoglobulin subclass deficiency: response to intravenous immunoglobulin therapy
Abstract
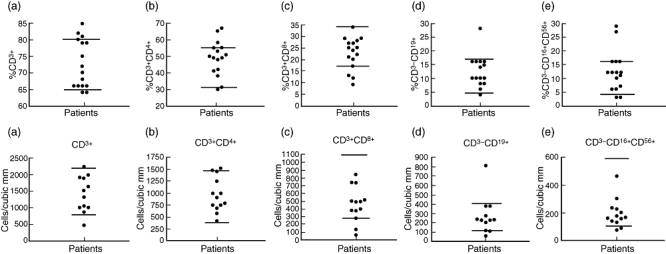
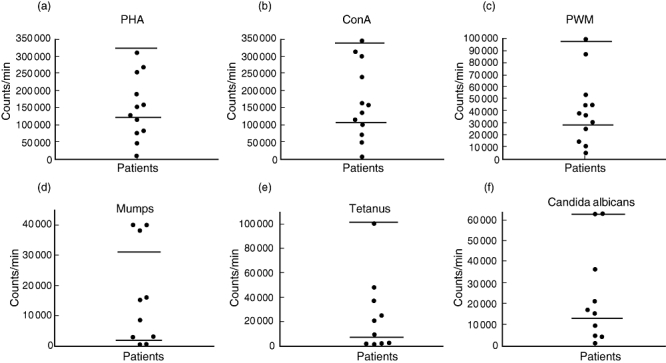
Selective immunoglobulin (Ig)G3 subclass deficiency in adults, especially its immunological profile, has not been described previously in detail. Therefore, a retrospective chart review was conducted to characterize the immune profile and clinical manifestations in adult patients with selective IgG3 deficiency. We reviewed the charts of 17 adult patients attending our subspeciality immunology clinic with a diagnosis of selective IgG3 deficiency. The following immunological test results were recorded: lymphocyte subsets, proliferative response to mitogens (phytohaemagglutinin, concanavalin A, pokeweed mitogen) and soluble antigens (mumps, Candida albicans, tetanus toxoid), specific antibody response to tetanus toxoid and pneumococcal antigens, neutrophil oxidative burst and natural killer cell cytotoxicity. In addition, we recorded information about the types of infections and other associated diseases, and response to intravenous immunoglobulin therapy (IVIG). In the majority of patients, lymphocyte subsets were normal. Proliferative responses to mitogens and antigens were decreased in 33% and 40% of patients, respectively. Specific antibody responses to tetanus were normal; however, responses to various pneumococcal serotypes were impaired in a subset of patients. Patients suffered from recurrent upper respiratory tract infections, which usually decreased in frequency and severity following treatment with IVIG. The majority of these patients also had concurrent atopic diseases in the form of allergic rhinitis or asthma. Selective IgG3 subclass deficiency should be considered in adults with recurrent upper respiratory tract infections with or without allergic rhinitis or asthma, who may have normal levels of total IgG. IVIG appears to be an effective therapy.
Figures
References
-
- Buckley RH. Immunoglobulin G subclass deficiency: fact or fancy? Curr Allergy Asthma Rep. 2002;2:356–60. - PubMed
-
- Shackelford PG. IgG subclasses: importance in pediatric practice. Pediatr Rev. 1993;14:291–6. - PubMed
-
- Oxelius VA, Hanson LA, Bjorkander J, et al. IgG3 deficiency: common in obstructive lung disease. Hereditary in families with immunodeficiency and autoimmune disease. Monogr Allergy. 1986;20:106–15. - PubMed
-
- Meyts I, Bossuyt X, Proesmans M, De B. Isolated IgG3 deficiency in children: to treat or not to treat? Case presentation and review of the literature. Pediatr Allergy Immunol. 2006;17:544–50. - PubMed
-
- Barlan IB, Geha RS, Schneider LC. Therapy for patients with recurrent infections and low serum IgG3 levels. J Allergy Clin Immunol. 1993;92:353–5. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
