

Clinical effects of laparotomy with perioperative continuous peritoneal lavage and postoperative hemofiltration in patients with severe acute pancreatitis
- PMID: 20015376
- PMCID: PMC2803451
- DOI: 10.1186/1749-7922-4-45
Clinical effects of laparotomy with perioperative continuous peritoneal lavage and postoperative hemofiltration in patients with severe acute pancreatitis
Abstract
Background: The elevated serum and peritoneal cytokine concentrations responsible for the systemic response syndrome (SIRS) and multiorgan failure in patients with severe acute pancreatitis lead to high morbidity and mortality rates. Prompted by reports underlining the importance of reducing circulating inflammatory mediators in severe acute pancreatitis, we designed this study to evaluate the efficiency of laparotomy followed by continuous perioperative peritoneal lavage combined with postoperative continuous venovenous diahemofiltration (CVVDH) in managing critically ill patients refractory to intensive care therapy. As the major clinical outcome variables we measured morbidity, mortality and changes in the Acute Physiology and Chronic Health Evaluation (APACHE II) score and cytokine concentrations in serum and peritoneal lavage fluid over time.
Methods: From a consecutive group of 23 patients hospitalized for acute pancreatitis, we studied 6 patients all with Apache II scores >/=19, who underwent emergency surgery for acute complications (5 for an abdominal compartment syndrome and 1 for septic shock) followed by continuous perioperative peritoneal lavage and postoperative CVVDH. CVVDH was started within 12 hours after surgery and maintained for at least 72 hours, until the multiorgan dysfunction syndrome improved. Samples were collected from serum, peritoneal lavage fluid and CVVDH dialysate for cytokine assay. Apache II scores were measured daily and their association with cytokine levels was assessed.
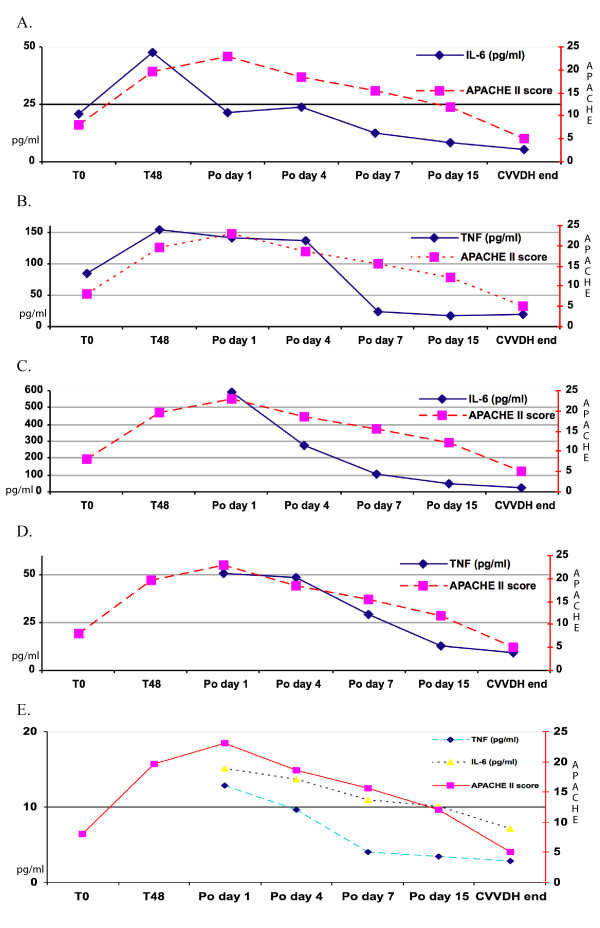
Results: All six patients tolerated CVVDH well, and the procedure lasted a mean 6 days (range, 3-12). Five patients survived and one died of Acinetobacter infection after surgery (mortality rate 16.6%). The mean APACHE II score was >/= 19 (range 19-22) before laparotomy and decreased significantly during peritoneal lavage and postoperative CVVDH (P = 0.013 by matched-pairs Students t-test). The decrease in cytokine concentrations in serum and lavage fluid was associated with the decrease in APACHE II scores and high interleukin 6 (IL-6) and tumor necrosis factor (TNF) concentrations in the hemofiltrate.
Conclusion: In critically ill patients with abdominal compartment syndrome, septic shock or high APACHE II scores related to severe acute pancreatitis, combining emergency laparotomy with continuous perioperative peritoneal lavage followed by postoperative CVVHD effectively reduces the local and systemic cytokines responsible for multiorgan dysfunction syndrome thus improving patients' outcome.
Figures
Similar articles
-
Effect of Laparoscopic Peritoneal Lavage and Drainage and Continuous Venovenous Diahemofiltration on Severe Acute Pancreatitis.J Laparoendosc Adv Surg Tech A. 2017 Nov;27(11):1145-1150. doi: 10.1089/lap.2016.0637. Epub 2017 Jun 6. J Laparoendosc Adv Surg Tech A. 2017. PMID: 28586262 Clinical Trial.
-
Improvement of monocyte function and immune homeostasis by high volume continuous venovenous hemofiltration in patients with severe acute pancreatitis.Int J Artif Organs. 2008 Oct;31(10):882-90. doi: 10.1177/039139880803101004. Int J Artif Organs. 2008. PMID: 19009506
-
Clinical Evaluation of Continuous Renal Replacement Therapy Combined with Peritoneal Lavage for Severe Acute Pancreatitis: A Retrospective Cohort Study.Med Sci Monit. 2023 Apr 12;29:e939314. doi: 10.12659/MSM.939314. Med Sci Monit. 2023. PMID: 37041732 Free PMC article.
-
Interleukin-6 and interleukin-8 extraction during continuous venovenous hemodiafiltration in septic acute renal failure.Ren Fail. 1995 Jul;17(4):457-66. doi: 10.3109/08860229509037609. Ren Fail. 1995. PMID: 7569116
-
Ascites fluid in severe acute pancreatitis: from pathophysiology to therapy.Acta Gastroenterol Belg. 2000 Jul-Sep;63(3):264-8. Acta Gastroenterol Belg. 2000. PMID: 11189983 Review.
Cited by
-
Effect of Early Continuous Veno-Venous Haemofiltration in Severe Acute Pancreatitis for the Prevention of Local Pancreatic Complications.Gastroenterol Res Pract. 2022 Mar 7;2022:7575231. doi: 10.1155/2022/7575231. eCollection 2022. Gastroenterol Res Pract. 2022. PMID: 35296066 Free PMC article.
-
The unrestricted global effort to complete the COOL trial.World J Emerg Surg. 2023 May 11;18(1):33. doi: 10.1186/s13017-023-00500-z. World J Emerg Surg. 2023. PMID: 37170123 Free PMC article. Clinical Trial.
-
Prior peritoneal lavage with hot 0.9 % saline induces HSP70 expression and protects against cerulein-induced acute pancreatitis in rats.Mol Biol Rep. 2013 Feb;40(2):1443-9. doi: 10.1007/s11033-012-2187-6. Epub 2012 Oct 21. Mol Biol Rep. 2013. PMID: 23096089
-
Embryonic natural orifice transluminal endoscopic surgery in the treatment of severe acute pancreatitis complicated by abdominal compartment syndrome.World J Emerg Med. 2015;6(1):23-8. doi: 10.5847/wjem.j.1920-8642.2015.01.004. World J Emerg Med. 2015. PMID: 25802562 Free PMC article.
-
A prolonged multispecies outbreak of IMP-6 carbapenemase-producing Enterobacterales due to horizontal transmission of the IncN plasmid.Sci Rep. 2020 Mar 5;10(1):4139. doi: 10.1038/s41598-020-60659-2. Sci Rep. 2020. PMID: 32139745 Free PMC article.
References
-
- Dugernier T, Starkel P, Laterre PF, Reynaert MS. Severe acute pancreatitis: pathophysiologic mechanisms underlying pancreatic necrosis and remote organ damage. Acta Gastroenterol Belg. 1996;59:178–185. - PubMed
LinkOut - more resources
Full Text Sources
Medical
Research Materials
