

Stainless steel ions stimulate increased thrombospondin-1-dependent TGF-beta activation by vascular smooth muscle cells: implications for in-stent restenosis
- PMID: 20016205
- PMCID: PMC2895758
- DOI: 10.1159/000265565
Stainless steel ions stimulate increased thrombospondin-1-dependent TGF-beta activation by vascular smooth muscle cells: implications for in-stent restenosis
Abstract
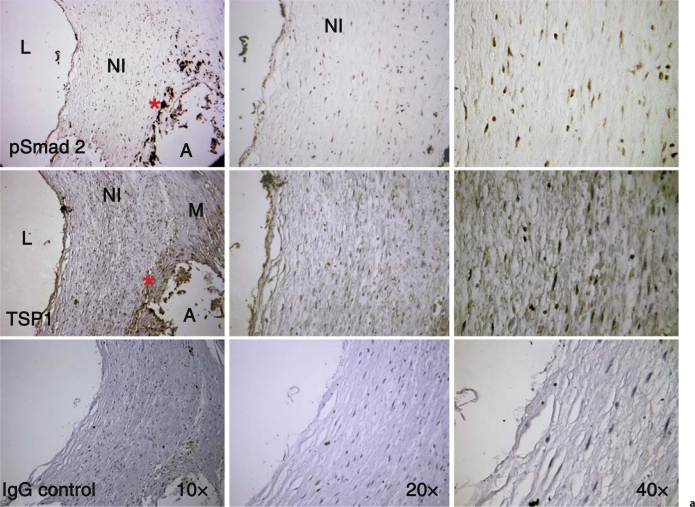
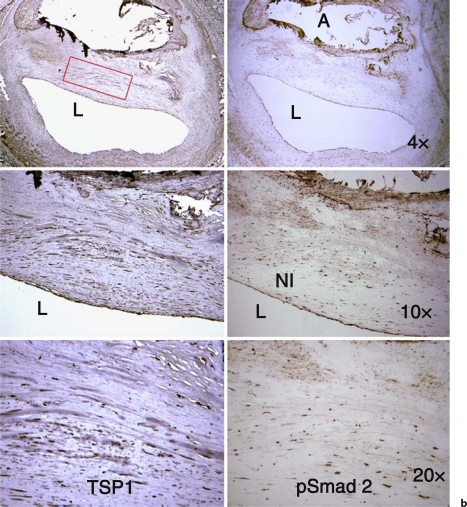
Background/aims: Despite advances in stent design, in-stent restenosis (ISR) remains a significant clinical problem. All implant metals exhibit corrosion, which results in release of metal ions. Stainless steel (SS), a metal alloy widely used in stents, releases ions to the vessel wall and induces reactive oxygen species, inflammation and fibroproliferative responses. The molecular mechanisms are unknown. TGF-beta is known to be involved in the fibroproliferative responses of vascular smooth muscle cells (VSMCs) in restenosis, and TGF-beta antagonists attenuate ISR. We hypothesized that SS ions induce the latent TGF-beta activator, thrombospondin-1 (TSP1), through altered oxidative signaling to stimulate increased TGF-beta activation and VSMC phenotype change.
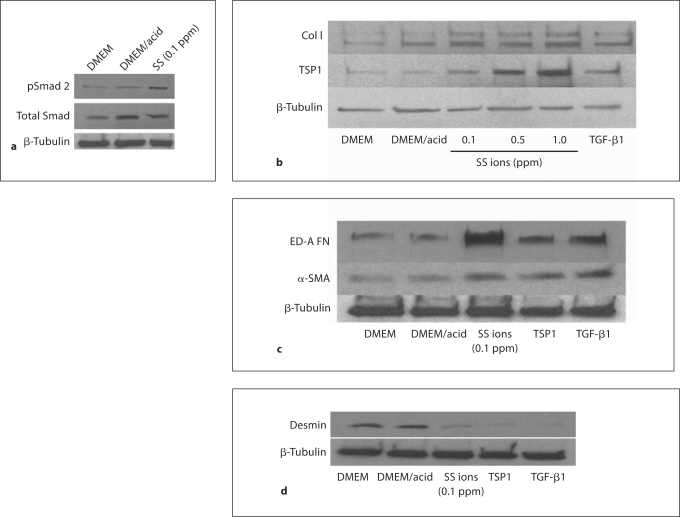
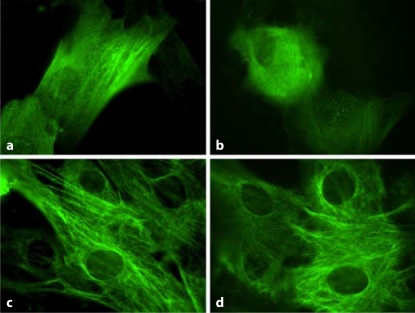
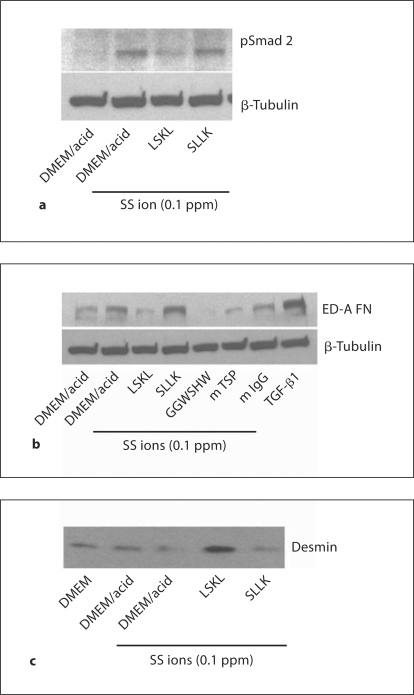
Methods: VSMCs were treated with SS metal ion cocktails, and morphology, TSP1, extracellular matrix production, desmin and TGF-beta activity were assessed by immunoblotting.
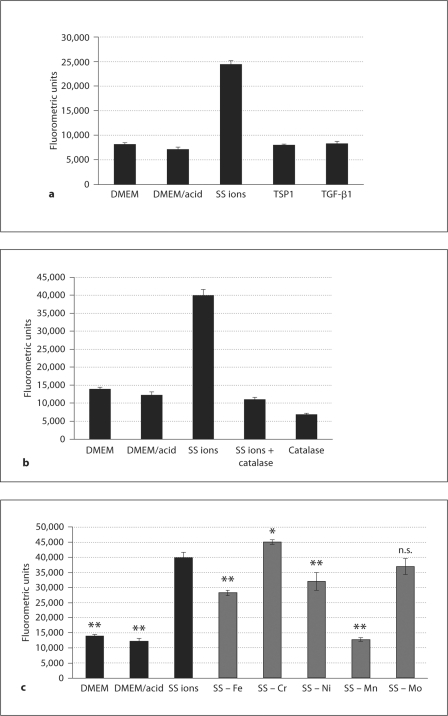
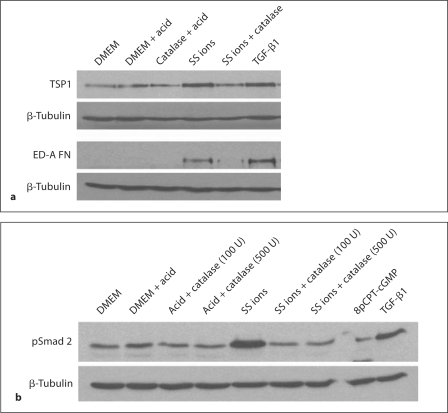
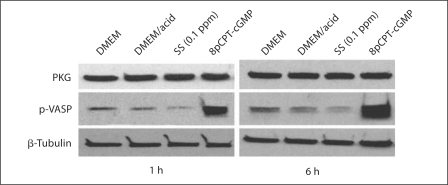
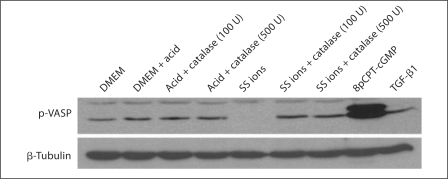
Results: SS ions stimulate the synthetic phenotype, increased TGF-beta activity, TSP1, increased extracellular matrix and downregulation of desmin in VSMCs. Furthermore, SS ions increase hydrogen peroxide and decrease cGMP-dependent protein kinase (PKG) signaling, a known repressor of TSP1 transcription. Catalase blocks SS ion attenuation of PKG signaling and increased TSP1 expression.
Conclusions: These data suggest that ions from stent alloy corrosion contribute to ISR through stimulation of TSP1-dependent TGF-beta activation.
Copyright 2009 S. Karger AG, Basel.
Figures
References
-
- Scott NA. Restenosis following implantation of bare metal coronary stents: Pathophysiology and pathways involved in the vascular response to injury. Adv Drug Deliv Rev. 2006;58:358–376. - PubMed
-
- Santin M, Colombo P, Bruschi G. Interfacial biology of in-stent restenosis. Expert Rev Med Devices. 2005;2:429–443. - PubMed
-
- Celik T, Iyisoy A, Jata B, Yuksel CU, Isik E. Stent fracture: a new villain of the village. Int J Cardiol. 2008 E-pub ahead of print. - PubMed
-
- Kim JS, Lee SY, Lee JM, Yoon YW, Ahn CM, Kim MH, Min PK, Ko YG, Hong BK, Choi D, Kwon HM, Jang Y, Shim WH. Significant association of coronary stent fracture with in-stent restenosis in sirolimus-eluting stents. Coron Artery Dis. 2009;20:59–63. - PubMed
-
- Rits J, van Herwaarden JA, Jahrome AK, Krievins D, Moll FL. The incidence of arterial stent fractures with exclusion of coronary, aortic, and non-arterial settings. Eur J Vasc Endovasc Surg. 2008;36:339–345. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- EB001715/EB/NIBIB NIH HHS/United States
- F30 DE018259/DE/NIDCR NIH HHS/United States
- HL044195/HL/NHLBI NIH HHS/United States
- R01 HL080017/HL/NHLBI NIH HHS/United States
- HL080017/HL/NHLBI NIH HHS/United States
- F30DE018259/DE/NIDCR NIH HHS/United States
- C06 RR 15490/RR/NCRR NIH HHS/United States
- C06 RR015490/RR/NCRR NIH HHS/United States
- R01 EB001715/EB/NIBIB NIH HHS/United States
- HL079644/HL/NHLBI NIH HHS/United States
- R01 HL079644/HL/NHLBI NIH HHS/United States
- DK078038/DK/NIDDK NIH HHS/United States
- R01 DK060658/DK/NIDDK NIH HHS/United States
- R01 DK078038/DK/NIDDK NIH HHS/United States
- R01 HL044195/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Miscellaneous
