

Enhanced memory responses to seasonal H1N1 influenza vaccination of the skin with the use of vaccine-coated microneedles
- PMID: 20017632
- PMCID: PMC2798016
- DOI: 10.1086/649228
Enhanced memory responses to seasonal H1N1 influenza vaccination of the skin with the use of vaccine-coated microneedles
Abstract
Background: Morbidity and mortality due to influenza could be reduced by improved vaccination.
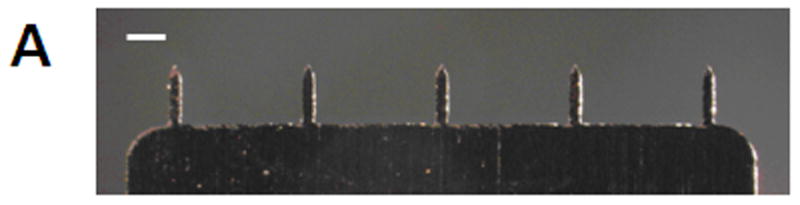
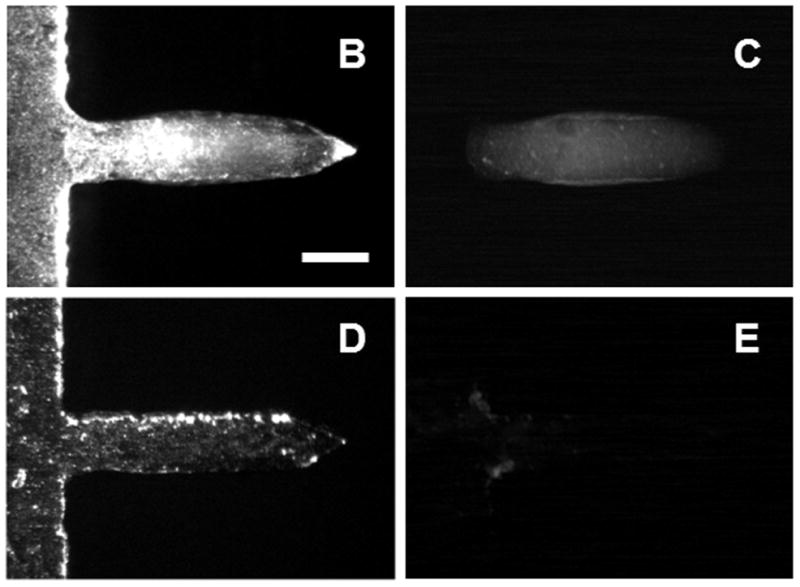
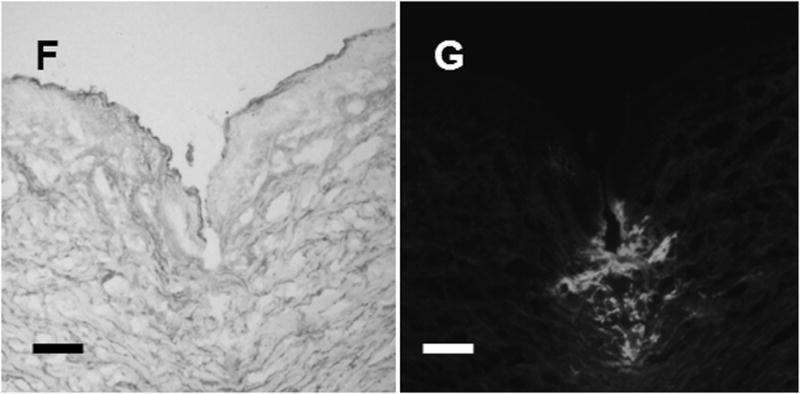
Methods: To develop a novel skin delivery method that is simple and allows for easy self-administration, we prepared microneedle patches with stabilized influenza vaccine and investigated their protective immune responses.
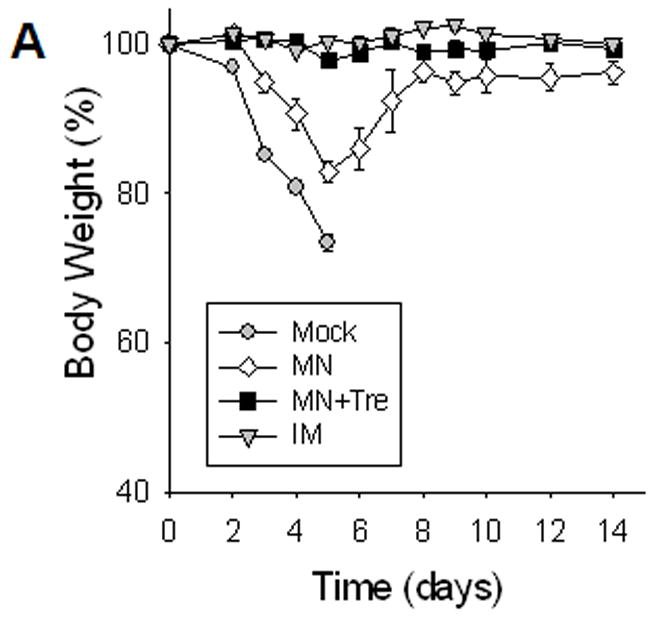
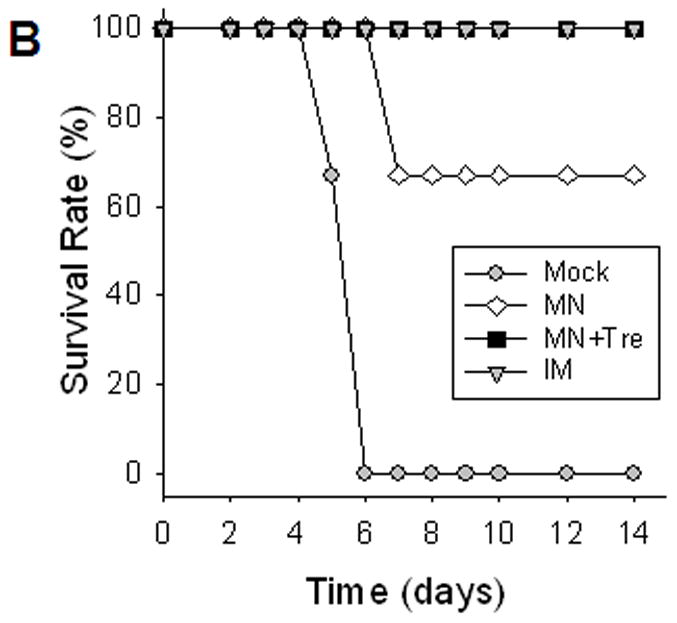
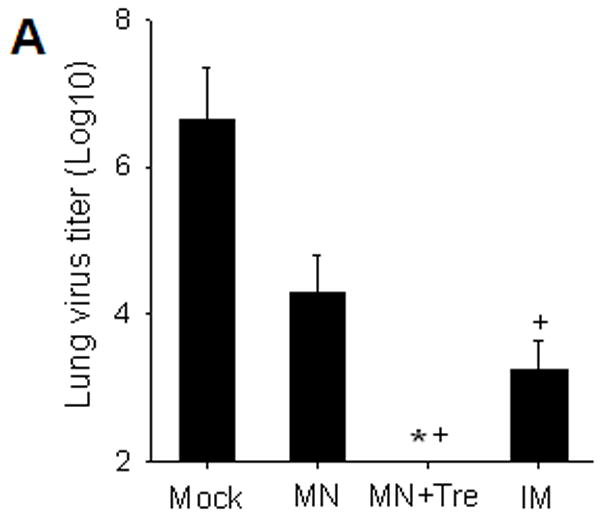
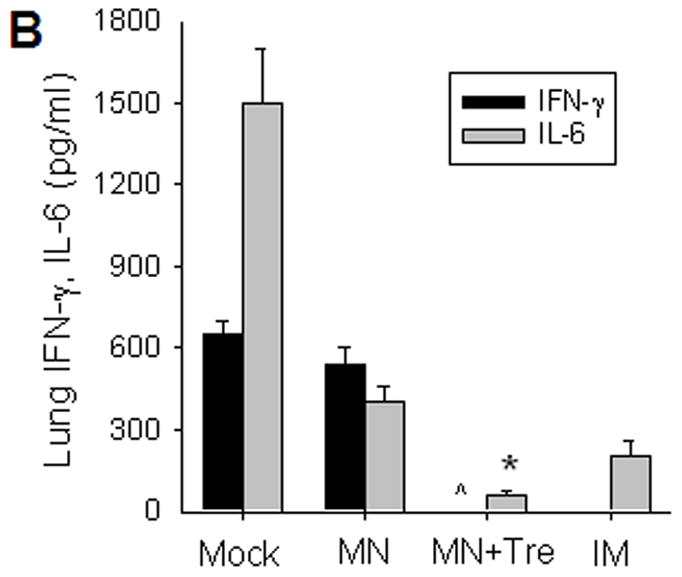
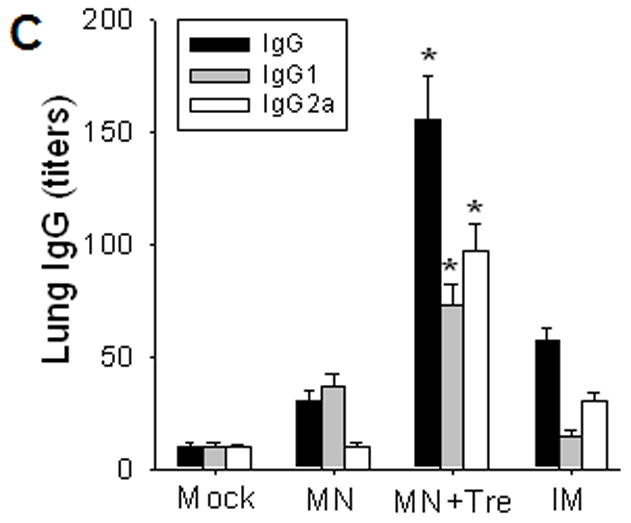
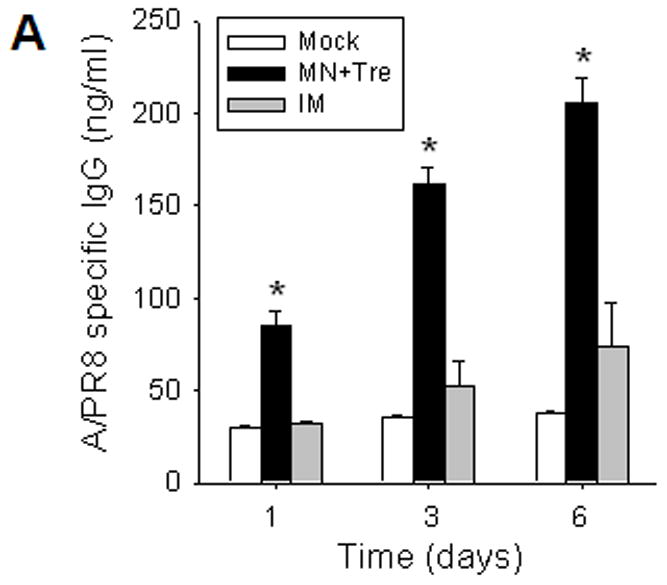
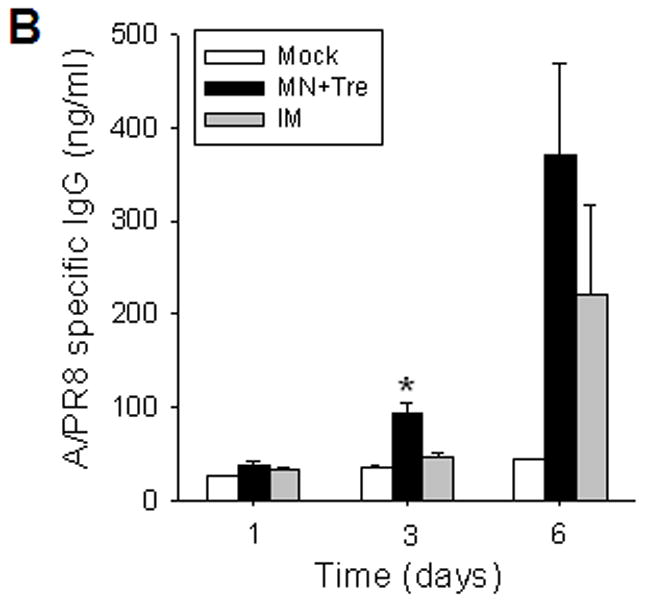
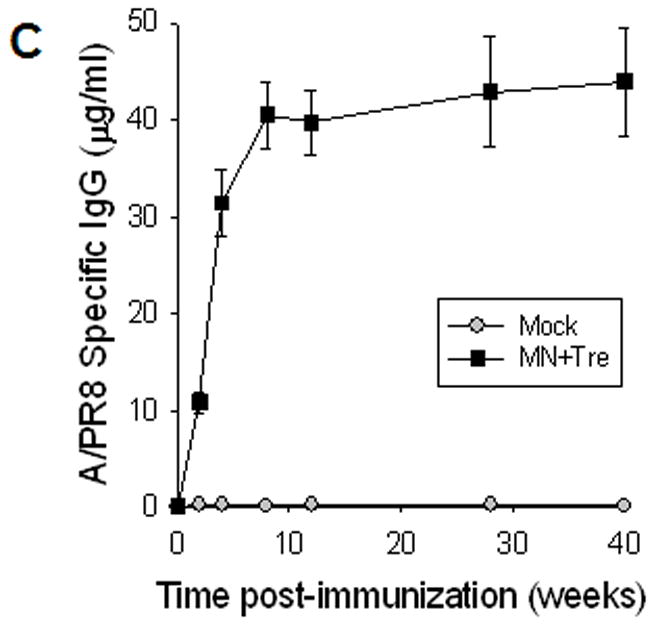
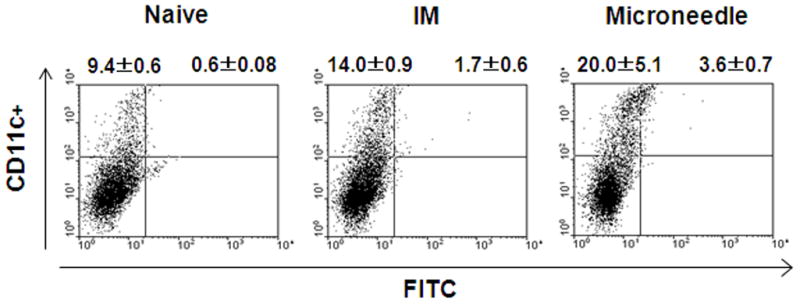
Results: Mice vaccinated with a single microneedle dose of trehalose-stabilized influenza vaccine developed strong antibody responses that were long-lived. Compared with traditional intramuscular vaccination, stabilized microneedle vaccination was superior in inducing protective immunity, as was evidenced by efficient clearance of virus from the lung and enhanced humoral and antibody-secreting cell immune responses after 100% survival from lethal challenge. Vaccine stabilization was found to be important, because mice vaccinated with an unstabilized microneedle vaccine elicited a weaker immunoglobulin G 2a antibody response, compared with the stabilized microneedle vaccine, and were only partially protected against viral challenge. Improved trafficking of dendritic cells to regional lymph nodes as a result of microneedle delivery to the skin might play a role in contributing to improved protective immunity.
Conclusions: These findings suggest that vaccination of the skin using a microneedle patch can improve protective efficacy and induce long-term sustained immunogenicity and may also provide a simple method of administration to improve influenza vaccination coverage.
Conflict of interest statement
Figures
References
-
- Cox RJ, Brokstad KA, Ogra P. Influenza virus: Immunity and vaccination strategies. Comparison of the immune response to inactivated and live, attenuated influenza vaccines. Scandinavian J Immunol. 2004;59:1–15. - PubMed
-
- Palese P. Influenza: Old and new threats. Nat Med. 2004;10:S82–7. - PubMed
-
- Centers for Disease Control and Prevention. Prevention and control of influenza, recommendations of the Advisory Committee on Immunization Practices. Morbidity and Mortality Weekly Report. 2008;57:1–60. - PubMed
-
- Kermode M. Unsafe injections in low-income country health settings: need for injection safety promotion to prevent the spread of blood-borne viruses. Health Promot Int. 2004;19:95–103. - PubMed
-
- Mitragotri S. Immunization without needles. Nat Rev Immunol. 2005;5:905–16. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
