

Cutting edge: lymphatic vessels, not blood vessels, primarily mediate immune rejections after transplantation
- PMID: 20018627
- PMCID: PMC4725297
- DOI: 10.4049/jimmunol.0903180
Cutting edge: lymphatic vessels, not blood vessels, primarily mediate immune rejections after transplantation
Abstract
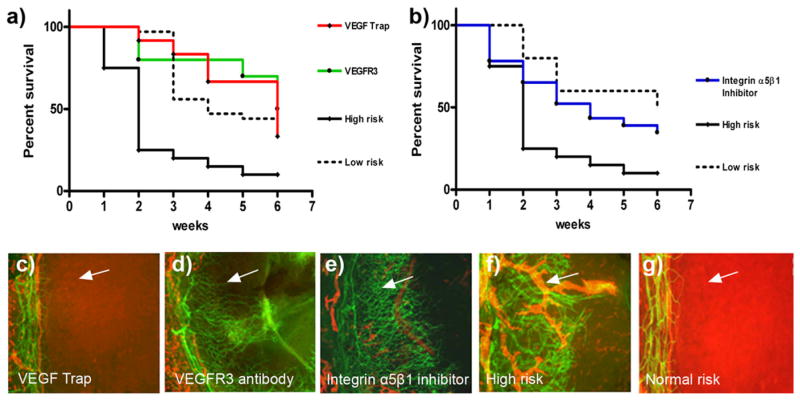
The purpose of this study was to determine the relative importance of blood vessels (hemangiogenesis) versus lymphatic vessels (lymphangiogenesis) in mediating immunological responses after transplantation. Using the murine model of corneal transplantation, graft survival was compared in differentially prevascularized and avascular recipient beds. Donor corneas (C57BL/6) were transplanted into uninflamed or inflamed avascular, prehemvascularized only or prehemvascularized and prelymphvascularized recipient murine eyes (BALB/C). Selective inhibition of lymphangiogenesis was achieved using antivascular endothelial growth factor receptor 3 Abs and anti-integrin alpha5 small molecules. Grafts placed into only prehemvascularized recipient beds had a similarly good graft survival compared with grafts placed into completely avascular, normal recipients, whereas the pre-existence of lymphatic vessels significantly deteriorated corneal graft survival (p < 0.05). Lymphatic vessels seem to contribute significantly to graft rejection after (corneal) transplantation. That may allow for selective, temporary, perioperative antilymphangiogenic treatment to promote graft survival without affecting blood vessels, even after solid organ transplantation.
Figures

References
-
- Lechler RI, Sykes M, Thomson AW, Turka LA. Organ transplantation—how much of the promise has been realized? Nat Med. 2005;11:605–613. - PubMed
-
- Kaplan HJ, Streilein JW, Stevens TR. Transplantation immunology of the anterior chamber of the eye. II. Immune response to allogeneic cells. J Immunol. 1975;115:805–810. - PubMed
-
- Kerjaschki D, Huttary N, Raab I, Regele H, Bojarski-Nagy K, Bartel G, Kröber SM, Greinix H, Rosenmaier A, Karlhofer F, et al. Lymphatic endothelial progenitor cells contribute to de novo lymphangiogenesis in human renal transplants. Nat Med. 2006;12:230–234. - PubMed
-
- Yamamoto I, Yamaguchi Y, Yamamoto H, Hosoya T, Horita S, Tanabe K, Fuchinoue S, Teraoka S, Toma H. A pathological analysis of lymphatic vessels in early renal allograft. Transplant Proc. 2006;38:3300–3303. - PubMed
-
- Stuht S, Gwinner W, Franz I, Schwarz A, Jonigk D, Kreipe H, Kerjaschki D, Haller H, Mengel M. Lymphatic neoangiogenesis in human renal allografts: results from sequential protocol biopsies. Am J Transplant. 2007;7:377–384. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
