

A prospective trial of 3T and 1.5T time-of-flight and contrast-enhanced MR angiography in the follow-up of coiled intracranial aneurysms
- PMID: 20019107
- PMCID: PMC7964181
- DOI: 10.3174/ajnr.A1932
A prospective trial of 3T and 1.5T time-of-flight and contrast-enhanced MR angiography in the follow-up of coiled intracranial aneurysms
Abstract
Background and purpose: Endovascularly coiled intracranial aneurysms are increasingly being followed up with noninvasive MRA imaging to evaluate for aneurysm recurrences. It has not been well-established which MRA techniques are best for this application, however. Our aim was to prospectively compare 4 MRA techniques, TOF and CE-MRA at 1.5T and 3T, to a reference standard of DSA in the evaluation of previously endovascularly coiled intracranial aneurysms.
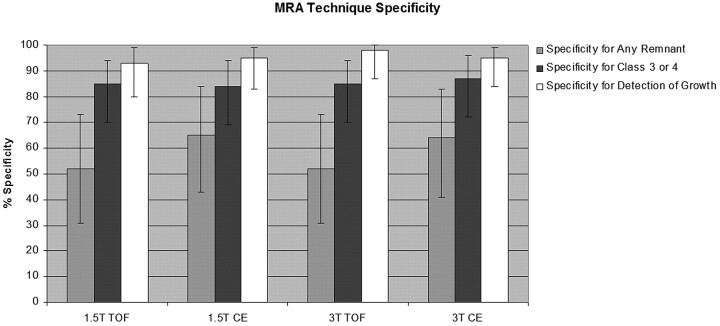
Materials and methods: Fifty-eight subjects with 63 previously coiled intracranial aneurysms underwent all 4 MRA techniques within 8 days of DSA. There were 2 outcome variables: coil occlusion class (class 1, complete; class 2, dog ear; class 3, residual neck; class 4, aneurysm filling) and change in degree of occlusion since the previous comparison. Sensitivity and specificity were computed for each MRA technique relative to the reference standard of DSA. Differences among the MRA techniques were evaluated in pair-wise fashion by using the McNemar test.
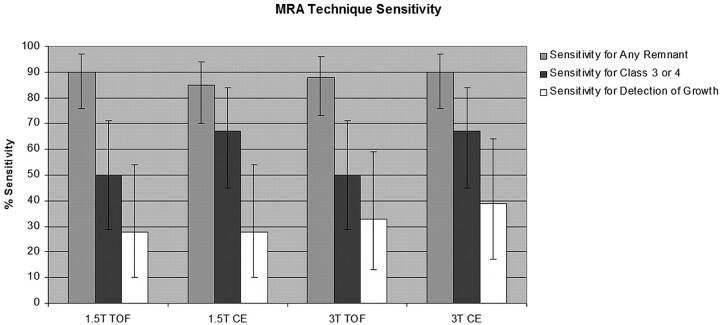
Results: For the detection of any aneurysm remnant, the sensitivity was 85%-90% for all MRA techniques. Sensitivity dropped to 50%-67% when calculated for the detection of only the class 3 and 4 aneurysm remnants, because several class 3 and 4 remnants were misclassified as class 2 by MRA. CE-MRA at 1.5T and 3T misclassified fewer of the class 3 and 4 remnants than did TOF-MRA at 1.5T, as reflected by the significantly greater sensitivity for larger aneurysm remnants with CE-MRA relative to TOF-MRA at 1.5T (P = .0455 for both comparisons).
Conclusions: CE-MRA is more likely than TOF-MRA to classify larger aneurysm remnants appropriately. We recommend performing both CE-MRA and TOF-MRA in the follow-up of coiled intracranial aneurysms and at 3T if available.
Figures
References
-
- Molyneux A, Kerr R, Stratton I, et al. . International Subarachnoid Aneurysm Trial (ISAT) of neurosurgical clipping versus endovascular coiling in 2143 patients with ruptured intracranial aneurysms: a randomised trial. Lancet 2002;360:1267–74 - PubMed
-
- Renowden SA, Benes V, Bradley M, et al. . Detachable coil embolisation of ruptured intracranial aneurysms: a single center study, a decade experience. Clin Neurol Neurosurg 2009;111:179–88. Epub 2008 Nov 13 - PubMed
-
- Molyneux AJ, Kerr RS, Yu LM, et al. . International subarachnoid aneurysm trial (ISAT) of neurosurgical clipping versus endovascular coiling in 2143 patients with ruptured intracranial aneurysms: a randomised comparison of effects on survival, dependency, seizures, rebleeding, subgroups, and aneurysm occlusion. Lancet 2005;366:809–17 - PubMed
-
- Kaufmann TJ, Huston J, 3rd, Mandrekar JN, et al. . Complications of diagnostic cerebral angiography: evaluation of 19,826 consecutive patients. Radiology 2007;243:812–19 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical