

Esophageal pressures in acute lung injury: do they represent artifact or useful information about transpulmonary pressure, chest wall mechanics, and lung stress?
- PMID: 20019160
- PMCID: PMC2838644
- DOI: 10.1152/japplphysiol.00835.2009
Esophageal pressures in acute lung injury: do they represent artifact or useful information about transpulmonary pressure, chest wall mechanics, and lung stress?
Abstract
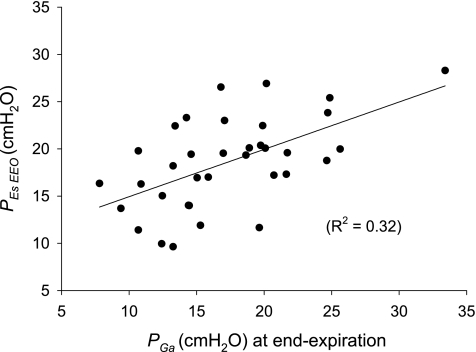
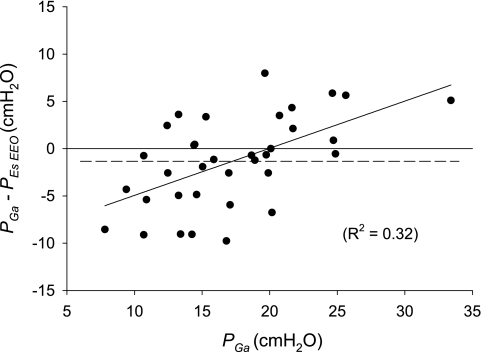
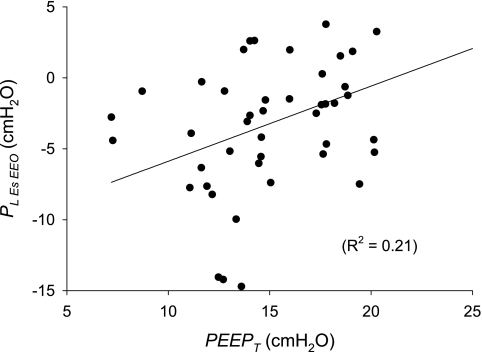
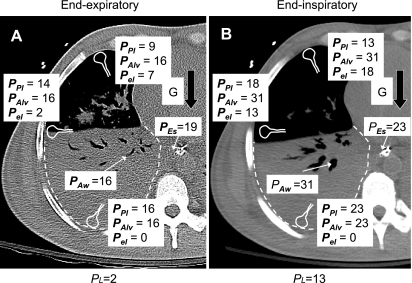
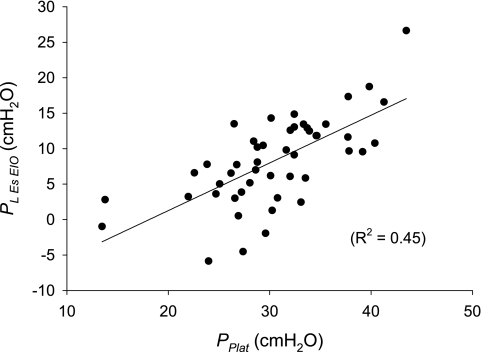
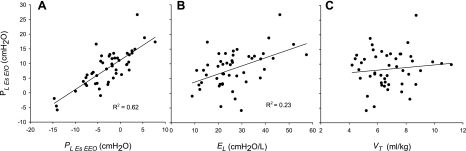
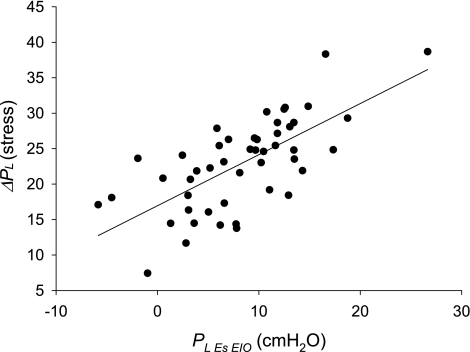
Acute lung injury can be worsened by inappropriate mechanical ventilation, and numerous experimental studies suggest that ventilator-induced lung injury is increased by excessive lung inflation at end inspiration or inadequate lung inflation at end expiration. Lung inflation depends not only on airway pressures from the ventilator but, also, pleural pressure within the chest wall. Although esophageal pressure (Pes) measurements are often used to estimate pleural pressures in healthy subjects and patients, they are widely mistrusted and rarely used in critical illness. To assess the credibility of Pes as an estimate of pleural pressure in critically ill patients, we compared Pes measurements in 48 patients with acute lung injury with simultaneously measured gastric and bladder pressures (Pga and P(blad)). End-expiratory Pes, Pga, and P(blad) were high and varied widely among patients, averaging 18.6 +/- 4.7, 18.4 +/- 5.6, and 19.3 +/- 7.8 cmH(2)O, respectively (mean +/- SD). End-expiratory Pes was correlated with Pga (P = 0.0004) and P(blad) (P = 0.0104) and unrelated to chest wall compliance. Pes-Pga differences were consistent with expected gravitational pressure gradients and transdiaphragmatic pressures. Transpulmonary pressure (airway pressure - Pes) was -2.8 +/- 4.9 cmH(2)O at end exhalation and 8.3 +/- 6.2 cmH(2)O at end inflation, values consistent with effects of mediastinal weight, gravitational gradients in pleural pressure, and airway closure at end exhalation. Lung parenchymal stress measured directly as end-inspiratory transpulmonary pressure was much less than stress inferred from the plateau airway pressures and lung and chest wall compliances. We suggest that Pes can be used to estimate transpulmonary pressures that are consistent with known physiology and can provide meaningful information, otherwise unavailable, in critically ill patients.
Figures
Comment in
-
Is there a place for esophageal manometry in the care of patients with injured lungs?J Appl Physiol (1985). 2010 Mar;108(3):481-2. doi: 10.1152/japplphysiol.00027.2010. Epub 2010 Jan 14. J Appl Physiol (1985). 2010. PMID: 20075267 No abstract available.
References
-
- Acute Respiratory Distress Syndrome Network Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. N Engl J Med 342: 1301–1308, 2000 - PubMed
-
- Anthonisen NR, Danson J, Robertson PC, Ross WR. Airway closure as a function of age. Respir Physiol 8: 58–65, 1969 - PubMed
-
- Bode FR, Dosman J, Martin RR, Ghezzo H, Macklem PT. Age and sex differences in lung elasticity and in closing capacity in nonsmokers. J Appl Physiol 41: 129–135, 1976 - PubMed
-
- Brander L, Ranieri VM, Slutsky AS. Esophageal and transpulmonary pressure help optimize mechanical ventilation in patients with acute lung injury. Crit Care Med 34: 1556–1558, 2006 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical