

Case Reports
doi: 10.1164/rccm.200907-1022CR.
Epub 2009 Dec 17.
Pulmonary alveolar proteinosis in workers at an indium processing facility
Affiliations
- PMID: 20019344
- PMCID: PMC3159086
- DOI: 10.1164/rccm.200907-1022CR
Item in Clipboard
Case Reports
Pulmonary alveolar proteinosis in workers at an indium processing facility
Am J Respir Crit Care Med.
.
Abstract
Two cases of pulmonary alveolar proteinosis, including one death, occurred in workers at a facility producing indium-tin oxide (ITO), a compound used in recent years to make flat panel displays. Both workers were exposed to airborne ITO dust and had indium in lung tissue specimens. One worker was tested for autoantibodies to granulocytemacrophage-colonystimulating factor (GM-CSF) and found to have an elevated level. These cases suggest that inhalational exposure to ITO causes pulmonary alveolar proteinosis, which may occur via an autoimmune mechanism.
Figures

High resolution computed tomography scan of the (A) left and (B) right chest showing bilateral ground glass opacities, centrilobular nodules, and intralobular and interlobular septal thickening. The changes were most prominent in the lower lobes.

High resolution computed tomography scan of the (A) left and (B) right chest showing bilateral ground glass opacities, centrilobular nodules, and intralobular and interlobular septal thickening. The changes were most prominent in the lower lobes.
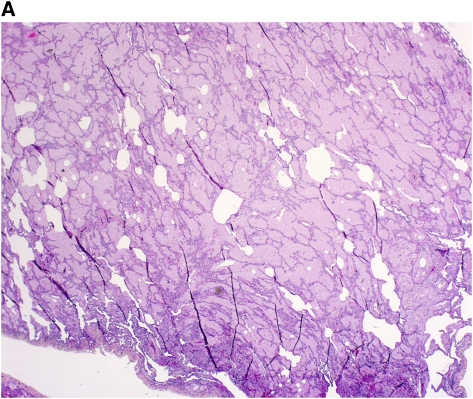
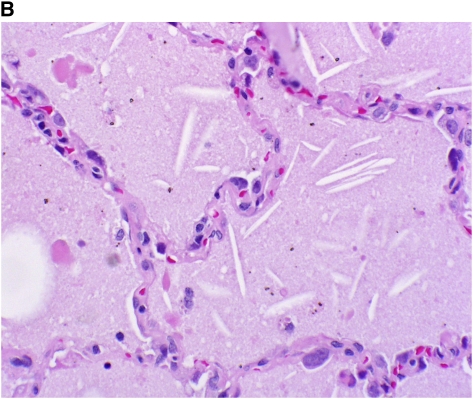
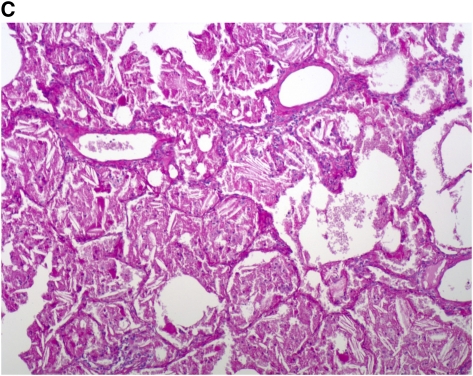
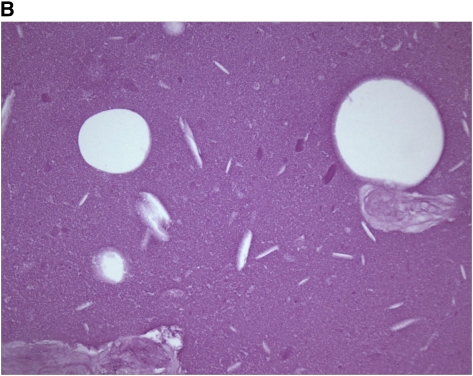
Histopathological sections of lung biopsy, hematoxylin and eosin stain. (A) Low-power overview showing filling of alveolar spaces by eosinophilic material (magnification ×10). (B) High-power view showing granular eosinophilic material and cholesterol clefts. Note the particulate material within the intraalveolar exudate (magnification ×200). Birefrigent particles were identified with polarizing microscopy, consistent with the presence of crystalline indium-tin oxide. (C) Periodic acid-Schiff (PAS) stain after diastase digestion, showing granular, PAS-positive intraalveolar material, and cholesterol clefts (magnification ×100).
Histopathological sections of lung biopsy, hematoxylin and eosin stain. (A) Low-power overview showing filling of alveolar spaces by eosinophilic material (magnification ×10). (B) High-power view showing granular eosinophilic material and cholesterol clefts. Note the particulate material within the intraalveolar exudate (magnification ×200). Birefrigent particles were identified with polarizing microscopy, consistent with the presence of crystalline indium-tin oxide. (C) Periodic acid-Schiff (PAS) stain after diastase digestion, showing granular, PAS-positive intraalveolar material, and cholesterol clefts (magnification ×100).
Histopathological sections of lung biopsy, hematoxylin and eosin stain. (A) Low-power overview showing filling of alveolar spaces by eosinophilic material (magnification ×10). (B) High-power view showing granular eosinophilic material and cholesterol clefts. Note the particulate material within the intraalveolar exudate (magnification ×200). Birefrigent particles were identified with polarizing microscopy, consistent with the presence of crystalline indium-tin oxide. (C) Periodic acid-Schiff (PAS) stain after diastase digestion, showing granular, PAS-positive intraalveolar material, and cholesterol clefts (magnification ×100).
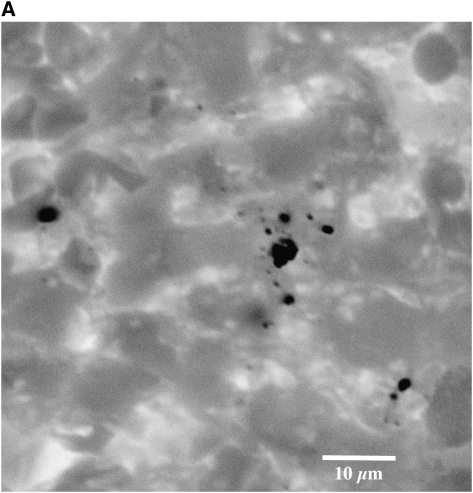
(A) Negative backscattered electron image obtained with the scanning electron microscope in an area of proteinosis shows numerous (dark) angulated particles within the respiratory size range (magnification ×2300). (B) Energy dispersive x-ray analyses of dozens of these particles identified only indium (In) and tin (Sn). A representative energy dispersive spectrum from one of these particles shows multiple peaks for In (including the small peak at 2.920 keV). There is overlap of the peaks between In and Sn, but the small right-most peak almost certainly represents Sn.
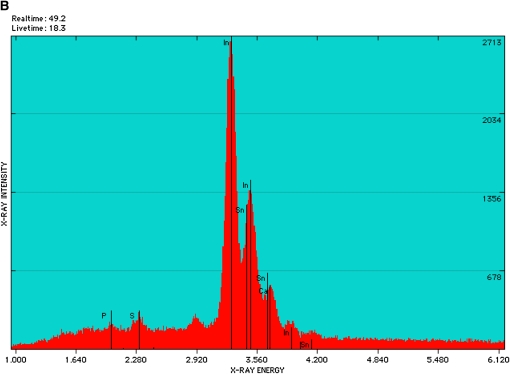
(A) Negative backscattered electron image obtained with the scanning electron microscope in an area of proteinosis shows numerous (dark) angulated particles within the respiratory size range (magnification ×2300). (B) Energy dispersive x-ray analyses of dozens of these particles identified only indium (In) and tin (Sn). A representative energy dispersive spectrum from one of these particles shows multiple peaks for In (including the small peak at 2.920 keV). There is overlap of the peaks between In and Sn, but the small right-most peak almost certainly represents Sn.
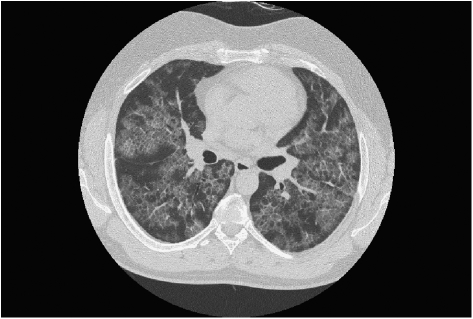
High resolution computed tomography scan of the chest showing bilateral alveolar ground-glass opacities and interstitial thickening in a mosaic pattern. These findings, commonly referred to as “crazy paving,” are consistent with, but not specific for, pulmonary alveolar proteinosis (10).
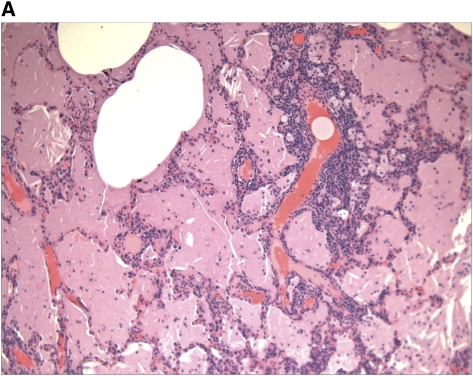
Histopathological sections of lung biopsy. (A) Hematoxylin and eosin stain showing filling of alveolar spaces with eosinophilic material (magnification ×40). (B) Periodic acid-Schiff (PAS) stain after diastase digestion, showing granular, PAS-positive intraalveolar material and cholesterol clefts (magnification ×400).
Histopathological sections of lung biopsy. (A) Hematoxylin and eosin stain showing filling of alveolar spaces with eosinophilic material (magnification ×40). (B) Periodic acid-Schiff (PAS) stain after diastase digestion, showing granular, PAS-positive intraalveolar material and cholesterol clefts (magnification ×400).
Comment in
-
Pulmonary alveolar proteinosis associated with dust inhalation: not secondary but autoimmune?Am J Respir Crit Care Med. 2010 Mar 1;181(5):427-8. doi: 10.1164/rccm.200912-1800ED. Am J Respir Crit Care Med. 2010. PMID: 20185750 No abstract available.
-
Pulmonary alveolar proteinosis in workers at an indium processing facility.Am J Respir Crit Care Med. 2010 Aug 15;182(4):578; author reply 578-9. doi: 10.1164/ajrccm.182.4.578. Am J Respir Crit Care Med. 2010. PMID: 20713641 No abstract available.
-
Indium-tin oxide does not induce GM-CSF autoantibodies.Am J Respir Crit Care Med. 2011 Sep 15;184(6):741; author reply 741-2. doi: 10.1164/ajrccm.184.6.741. Am J Respir Crit Care Med. 2011. PMID: 21920929 No abstract available.
References
-
- Homma T, Ueno T, Sekizawa K, Tanaka A, Hirata M. Interstial pneumonia developed in a worker dealing with particles containing indium-tin oxide. J Occup Health 2003;45:137–139. - PubMed
-
- Homma S, Miyamoto A, Sakamoto S, Kishi K, Motoi N, Yoshimura K. Pulmonary fibrosis in an individual occupationally exposed to inhaled indium-tin oxide. Eur Respir J 2005;25:200–204. - PubMed
-
- Watanabe WT, Ettensohn DB, Jhung JW, Roggli VL. Pulmonary alveolar proteinosis associated with occupational indium exposure [abstract]. Chest 2002;122:246S–247S.
-
- Medvedovski E, Alvarez N, Yankov O, Olsson MK. Advanced indium-tin oxide ceramics for sputtering targets. Ceram Int 2008;34:1173–1182.
-
- National Institute for Occupational Safety and Health (NIOSH). NIOSH pocket guide to chemical hazards. U.S. Department of Health and Human Services; 2005. DHHS Publication No. (NIOSH) 2005-149.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
