

Shared treatment decision making improves adherence and outcomes in poorly controlled asthma
- PMID: 20019345
- PMCID: PMC2841026
- DOI: 10.1164/rccm.200906-0907OC
Shared treatment decision making improves adherence and outcomes in poorly controlled asthma
Abstract
Rationale: Poor adherence to asthma controller medications results in poor treatment outcomes.
Objectives: To compare controller medication adherence and clinical outcomes in 612 adults with poorly controlled asthma randomized to one of two different treatment decision-making models or to usual care.
Methods: In shared decision making (SDM), nonphysician clinicians and patients negotiated a treatment regimen that accommodated patient goals and preferences. In clinician decision making, treatment was prescribed without specifically eliciting patient goals/preferences. The otherwise identical intervention protocols both provided asthma education and involved two in-person and three brief phone encounters.
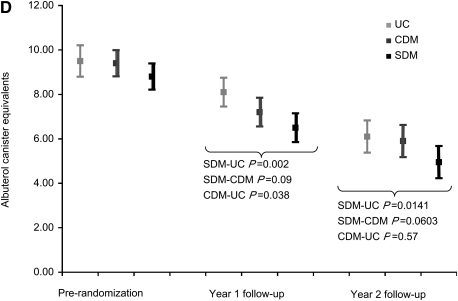
Measurements and main results: Refill adherence was measured using continuous medication acquisition (CMA) indices-the total days' supply acquired per year divided by 365 days. Cumulative controller medication dose was measured in beclomethasone canister equivalents. In follow-up Year 1, compared with usual care, SDM resulted in: significantly better controller adherence (CMA, 0.67 vs. 0.46; P < 0.0001) and long-acting beta-agonist adherence (CMA, 0.51 vs. 0.40; P = 0.0225); higher cumulative controller medication dose (canister equivalent, 10.9 vs. 5.2; P < 0.0001); significantly better clinical outcomes (asthma-related quality of life, health care use, rescue medication use, asthma control, and lung function). In Year 2, compared with usual care, SDM resulted in significantly lower rescue medication use, the sole clinical outcome available for that year. Compared with clinician decision making, SDM resulted in: significantly better controller adherence (CMA, 0.67 vs. 0.59; P = 0.03) and long-acting beta-agonist adherence (CMA, 0.51 vs. 0.41; P = 0.0143); higher cumulative controller dose (CMA, 10.9 vs. 9.1; P = 0.005); and quantitatively, but not significantly, better outcomes on all clinical measures.
Conclusions: Negotiating patients' treatment decisions significantly improves adherence to asthma pharmacotherapy and clinical outcomes. Clinical trials registered with www.clinicaltrials.gov (NCT00217945 and NCT00149526).
Figures










Comment in
-
Shared decisions making führt zu einer besseren Adherence und besseren Outcomes bei schlecht kontrolliertem Asthma.Praxis (Bern 1994). 2010 Sep 8;99(18):1111-2. doi: 10.1024/1661-8157/a000232. Praxis (Bern 1994). 2010. PMID: 20824615 German. No abstract available.
References
-
- Bosley CM, Parry DT, Cochrane GM. Patient compliance with inhaled medication: does combining beta-agonists with corticosteroids improve compliance? Eur Respir J 1994;7:504–509. - PubMed
-
- Sackett DL, Snow JC. The magnitude of compliance and non-compliance. In: Haynes RB, Taylor WD, Sackett DL, editors. Compliance in health care. Baltimore: Johns Hopkins University Press; 1979. pp. 11–22.
-
- Gong H, Simmons MS, Clark VA, Tashkin DP. Metered-dose inhaler usage in subjects with asthma: comparison of nebulizer chronolog and daily diary recordings. J Allergy Clin Immunol 1988;82:5–10. - PubMed
-
- Baum D, Creer TL. Medication compliance in children with asthma. J Asthma 1986;23:49–59. - PubMed
