

Identifying viral infections in vaccinated Chronic Obstructive Pulmonary Disease (COPD) patients using clinical features and inflammatory markers
- PMID: 20021505
- PMCID: PMC4941951
- DOI: 10.1111/j.1750-2659.2009.00113.x
Identifying viral infections in vaccinated Chronic Obstructive Pulmonary Disease (COPD) patients using clinical features and inflammatory markers
Abstract
Background: Known inflammatory markers have limited sensitivity and specificity to differentiate viral respiratory tract infections from other causes of acute exacerbation of COPD (AECOPD). To overcome this, we developed a multi-factorial prediction model combining viral symptoms with inflammatory markers.
Methods: Interleukin-6 (IL-6), serum amyloid A (SAA) and viral symptoms were measured in stable COPD and at AECOPD onset and compared with the viral detection rates on multiplex PCR. The predictive accuracy of each measure was assessed using logistic regression and receiver operating characteristics curve (ROC) analysis.
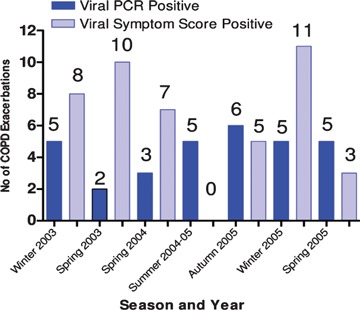
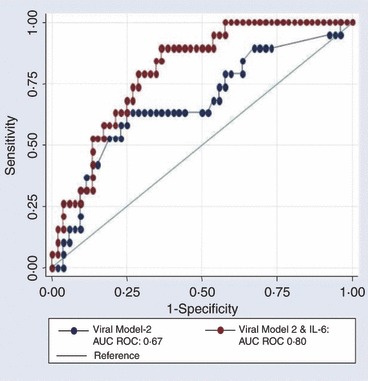
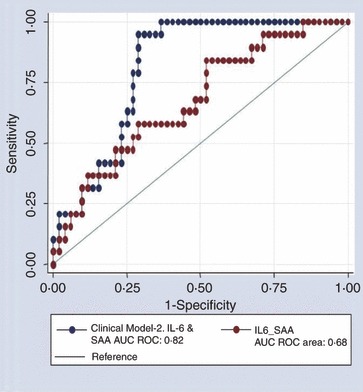
Results: There was a total of 33 viruses detected at the onset of 148 AECOPD, the majority 26 (79%) were picornavirus. Viral symptoms with the highest predictive values were rhinorrhoea [Odds ratio (OR) 4.52; 95% CI 1.99-10.29; P < 0.001] and sore throat (OR 2.64; 95% CI 1.14-6.08; P = 0.022), combined the AUC ROC curve was 0.67. At AECOPD onset patients experienced a 1.6-fold increase in IL-6 (P = 0.008) and 4.5-fold increase in SAA (P < 0.001). The addition of IL-6 to the above model significantly improved diagnostic accuracy compared with symptoms alone (AUC ROC 0.80 (P = 0.012).
Conclusion: The addition of inflammatory markers increases the specificity of a clinical case definition for viral infection, particularly picornavirus infection.
Figures
Similar articles
-
Correlations between serum amyloid A, C-reactive protein and clinical indices of patients with acutely exacerbated chronic obstructive pulmonary disease.J Clin Lab Anal. 2019 May;33(4):e22831. doi: 10.1002/jcla.22831. Epub 2019 Jan 21. J Clin Lab Anal. 2019. PMID: 30666727 Free PMC article.
-
[Respiratory virus infections and inflammatory cytokines in hospitalized patients with acute exacerbation of chronic obstructive pulmonary disease].Zhonghua Jie He He Hu Xi Za Zhi. 2018 Dec 12;41(12):942-948. doi: 10.3760/cma.j.issn.1001-0939.2018.12.009. Zhonghua Jie He He Hu Xi Za Zhi. 2018. PMID: 30522191 Chinese.
-
Analysis of viral infection and biomarkers in patients with acute exacerbation of chronic obstructive pulmonary disease.Clin Respir J. 2018 Mar;12(3):1228-1239. doi: 10.1111/crj.12656. Epub 2017 Jun 15. Clin Respir J. 2018. PMID: 28586150 Free PMC article.
-
Resolving Viral-Induced Secondary Bacterial Infection in COPD: A Concise Review.Front Immunol. 2018 Oct 16;9:2345. doi: 10.3389/fimmu.2018.02345. eCollection 2018. Front Immunol. 2018. PMID: 30459754 Free PMC article. Review.
-
Role of viruses in exacerbations of chronic obstructive pulmonary disease.Proc Am Thorac Soc. 2004;1(2):115-20. doi: 10.1513/pats.2306030. Proc Am Thorac Soc. 2004. PMID: 16113423 Review.
Cited by
-
Bronchiectasis exacerbation study on azithromycin and amoxycillin-clavulanate for respiratory exacerbations in children (BEST-2): study protocol for a randomized controlled trial.Trials. 2013 Feb 20;14:53. doi: 10.1186/1745-6215-14-53. Trials. 2013. PMID: 23421781 Free PMC article. Clinical Trial.
-
The influence of virus infections on the course of COPD.Eur J Microbiol Immunol (Bp). 2012 Sep;2(3):176-85. doi: 10.1556/EuJMI.2.2012.3.2. Epub 2012 Sep 10. Eur J Microbiol Immunol (Bp). 2012. PMID: 24688763 Free PMC article. Review.
-
Microbiological study of patients hospitalized for acute exacerbation of chronic obstructive pulmonary disease (AE-COPD) and the usefulness of analytical and clinical parameters in its identification (VIRAE study).Int J Chron Obstruct Pulmon Dis. 2012;7:327-35. doi: 10.2147/COPD.S30568. Epub 2012 May 25. Int J Chron Obstruct Pulmon Dis. 2012. PMID: 22745532 Free PMC article.
-
Antibiotics for bronchiectasis exacerbations in children: rationale and study protocol for a randomised placebo-controlled trial.Trials. 2012 Aug 31;13:156. doi: 10.1186/1745-6215-13-156. Trials. 2012. PMID: 22937736 Free PMC article. Clinical Trial.
-
Serum Amyloid A in Stable Patients with Chronic Obstructive Pulmonary Disease Does Not Reflect the Clinical Course of the Disease.Int J Mol Sci. 2023 Jan 27;24(3):2478. doi: 10.3390/ijms24032478. Int J Mol Sci. 2023. PMID: 36768801 Free PMC article.
References
-
- Hutchinson A., Ghimire AK, Thompson MA et al. A community‐based, time‐matched, case‐control study of respiratory viruses and exacerbations of COPD. Respir Med 2007; 101:2472–2481. - PubMed
-
- Seemungal T, Wedzicha J. Viral infections in obstructive airway diseases. Curr Opin Pulm Med 2003; 9:111–116. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
