

Diagnostic performance of multisequential cardiac magnetic resonance imaging in acute cardiac allograft rejection
- PMID: 20023044
- PMCID: PMC2796145
- DOI: 10.1093/eurjhf/hfp174
Diagnostic performance of multisequential cardiac magnetic resonance imaging in acute cardiac allograft rejection
Abstract
Aims: We evaluated cardiac magnetic resonance imaging (CMR) as a non-invasive test for cardiac allograft rejection.
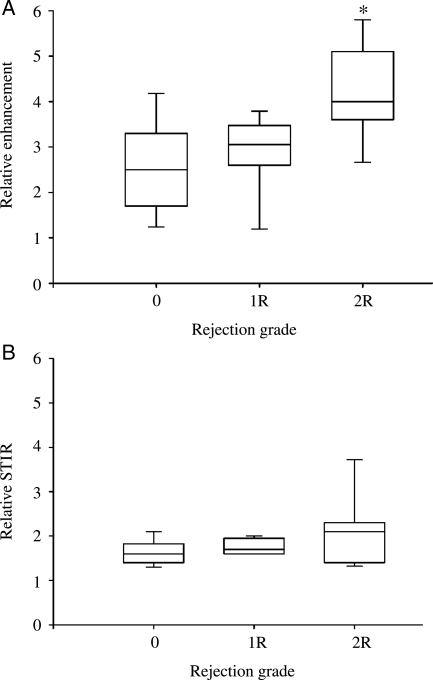
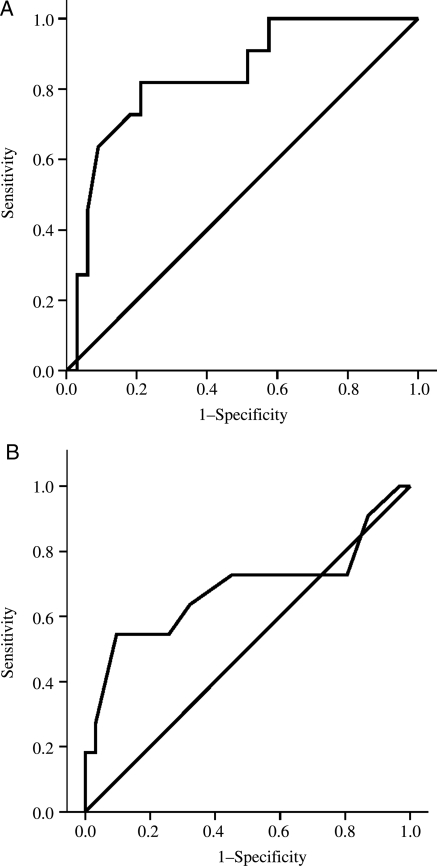
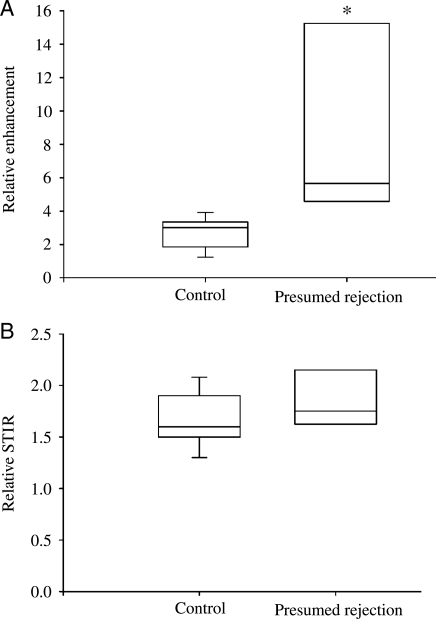
Methods and results: We performed CMR on 50 heart-transplant recipients. Acute rejection was confirmed in 11 cases by endomyocardial biopsy (EMB) and presumed in 8 cases with a recent fall in left-ventricular ejection fraction (LVEF) not attributable to coronary allograft vasculopathy. Control patients had both normal LVEF and no significant rejection on EMB. Cardiac magnetic resonance imaging evaluated myocardial function, oedema, and early and late post-Gadolinium-DTPA contrast enhancement. Patients with confirmed rejection demonstrated elevated early relative myocardial contrast enhancement (4.1 +/- 0.3 vs. 2.8 +/- 0.2, P < 0.001) and a trend to higher oedema suggested by higher relative myocardial intensity on T(2)-weighted imaging compared to controls (2.1 +/- 0.1 vs. 1.7 +/- 0.1, P = 0.1). With rejection defined as increased early contrast enhancement or myocardial oedema, the sensitivity and specificity of CMR compared with EMB were 100 and 73%, respectively. Eight patients with presumed rejection also had elevated early myocardial contrast enhancement compared with controls, (8.7 +/- 1.9 vs. 2.8 +/- 0.2, P < 0.05), which reduced following increased immunosuppression (8.7 +/- 1.9 vs. 4.6 +/- 1.2, P < 0.05). In these patients LVEF improved following increased immunosuppression (32 +/- 5 vs. 46 +/- 5%, P < 0.05).
Conclusion: Cardiac magnetic resonance imaging is a promising modality for non-invasive detection of cardiac allograft rejection.
Figures
References
-
- Fisher DC, Lake KD, Reutzel TJ, Emery RW. Changes in health-related quality of life and depression in heart transplant recipients. J Heart Lung Transplant. 1995;14:373–381. - PubMed
-
- Lindenfeld J, Miller GG, Shakar SF, Zolty R, Lowes BD, Wolfel EE, Mestroni L, Page RL, II, Kobashigawa J. Drug therapy in the heart transplant recipient: part I: cardiac rejection and immunosuppressive drugs. Circulation. 2004;110:3734–3740. - PubMed
-
- Hosenpud JD, Novick RJ, Breen TJ, Keck B, Daily P. The Registry of the International Society for Heart and Lung Transplantation: twelfth official report–1995. J Heart Lung Transplant. 1995;14:805–815. - PubMed
-
- White JA, Guiraudon C, Pflugfelder PW, Kostuk WJ. Routine surveillance myocardial biopsies are unnecessary beyond one year after heart transplantation. J Heart Lung Transplant. 1995;14:1052–1056. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
