

Intra-arterial chemotherapy with osmotic blood-brain barrier disruption for aggressive oligodendroglial tumors: results of a phase I study
- PMID: 20023537
- PMCID: PMC2806091
- DOI: 10.1227/01.
Intra-arterial chemotherapy with osmotic blood-brain barrier disruption for aggressive oligodendroglial tumors: results of a phase I study
Abstract
Objective: Refractory anaplastic oligodendroglioma and oligoastrocytoma tumors are challenging to treat. This trial primarily evaluated toxicity and estimated the maximum tolerated dose of intra-arterial (IA) melphalan, IA carboplatin, and intravenous (IV) etoposide phosphate in conjunction with blood-brain barrier disruption in these tumors. The secondary measure was efficacy.
Methods: Thirteen patients with temozolomide-refractory anaplastic oligodendroglioma (11 patients) or oligoastrocytoma (2 patients) underwent blood-brain barrier disruption with carboplatin (IA, 200 mg/m(2)/d), etoposide phosphate (IV, 200 mg/m(2)/d), and melphalan (IA, dose escalation) every 4 weeks, for up to 1 year. Patients underwent melphalan dose escalation (4, 8, 12, 16, and 20 mg/m(2)/d) until the maximum tolerated dose (1 level below that producing grade 4 toxicity) was determined. Toxicity and efficacy were assessed.
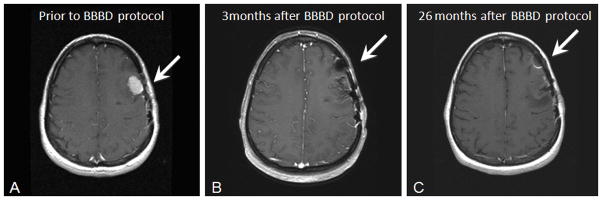
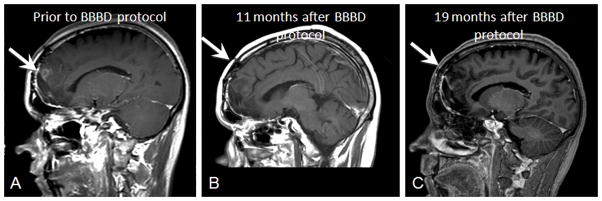
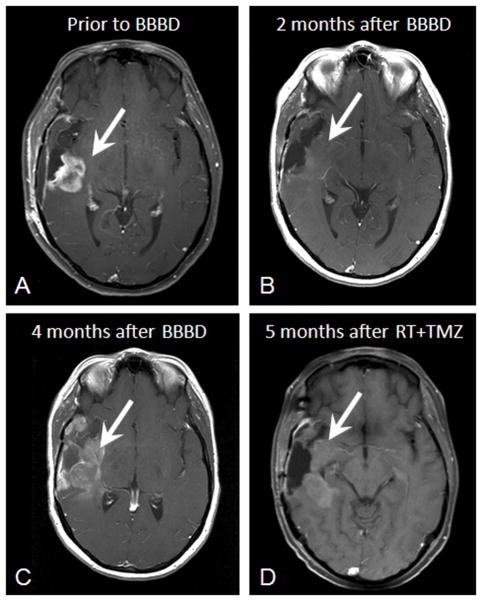
Results: Two of 4 patients receiving IA melphalan at 8 mg/m(2)/d developed grade 4 thrombocytopenia; thus, the melphalan maximum tolerated dose was 4 mg/m/d. Adverse events included asymptomatic subintimal tear (1 patient) and grade 4 thrombocytopenia (3 patients). Two patients demonstrated complete response, 3 had partial responses, 5 demonstrated stable disease, and 3 progressed. Median overall progression-free survival was 11 months. Patients with complete or partial response demonstrated deletion of chromosomes 1p and 19q. In the 5 patients with stable disease, 2 demonstrated 1p and 19q deletion, and 3 demonstrated 19q deletion only.
Conclusion: In patients with anaplastic oligodendroglioma or oligoastrocytoma tumors in whom temozolomide treatment has failed, osmotic blood-brain barrier disruption with IA carboplatin, IV etoposide phosphate, and IA melphalan (4 mg/m(2)/d for 2 days) shows acceptable toxicity and encouraging efficacy, especially in patients demonstrating 1p and/or 19q deletion.
Figures
References
-
- Guidelines for the audiologic management of individuals receiving cochleotoxic drug therapy. ASHA. 1994;36:11–19.
-
- Angelov L, Doolittle ND, Kraemer DF, Siegal T, Barnett GH, Peereboom DM, Stevens G, McGregor J, Jahnke K, Lacy C, Hedrick NA, Shalom E, Ference S, Bell S, Sorenson L, Tyson RM, Haluska M, Neuwelt E. Blood-brain barrier disruption and intra-arterial methotrexate-based therapy for newly diagnosed primary CNS lymphoma: a multi-institutional experience with 149 patients. J Clin Oncol. 2009 - PMC - PubMed
-
- Assietti R, Olson JJ. Intra-arterial cisplatin in malignant brain tumors: incidence and severity of otic toxicity. J Neurooncol. 1996;27:251–258. - PubMed
-
- Barth RF, Yang W, Rotaru JH, Moeschberger ML, Joel DD, Nawrocky MM, Goodman JH, Soloway AH. Boron neutron capture therapy of brain tumors: enhanced survival following intracarotid injection of either sodium borocaptate or boronophenylalanine with or without blood-brain barrier disruption. Cancer Res. 1997;57:1129–1136. - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
