

Vision loss after spinal fusion for scoliosis in a child with spinal cord injury
- PMID: 20025158
- PMCID: PMC2792468
- DOI: 10.1080/10790268.2009.11754567
Vision loss after spinal fusion for scoliosis in a child with spinal cord injury
Abstract
Background: Vision loss after spinal surgery is a rare and devastating complication. Risk factors include patient age, operative time, estimated blood loss, and intraoperative fluid management. Children with spinal cord injury often develop scoliosis that requires surgical correction.
Study design: Case report.
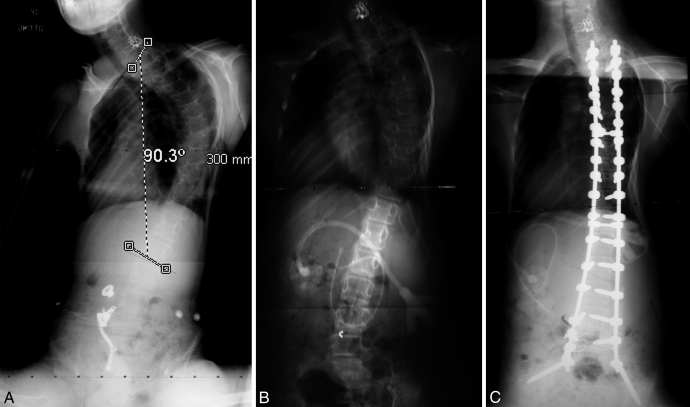
Methods: Clinical and radiographic review was conducted of a 15-year-old boy who developed severe scoliosis after sustaining a C5 level injury at age 4 years from a motor vehicle crash.
Findings: The patient underwent a posterior spinal fusion from T2 to the pelvis, and good correction of the spinal deformity was attained. During the 8-hour procedure, blood loss was 4000 mL (approximately 1.2 blood volumes) and 17,000 mL of fluids were administered. On postoperative day 5, it was determined that the patient had complete visual loss. Neuro-ophthalmology consultation confirmed the diagnosis of posterior ischemic optic neuropathy.
Conclusions: A significant number of children with spinal cord injury develop scoliosis requiring surgical correction. These procedures are often lengthy, with the potential for extensive blood loss and fluid shifts, factors that may increase the likelihood of postoperative vision loss. Patients should be counseled about this complication, and the surgical and anesthesiology teams should take all measures to minimize its occurrence.
Figures
References
-
- Dearolf WW, 3rd, Betz RR, Vogel LC. Effectiveness of spinal release and halo-femoral traction in the management of severe spinal deformity. J Pediatr Orthop. 1990;10(2):214–218. - PubMed
-
- Mehta S, Betz RR, Mulcahey MJ. Effect of bracing on paralytic scoliosis secondary to spinal cord injury. J Spinal Cord Med. 2004;27(suppl 1):S88–S92. - PubMed
-
- Tsirikos AI, Lipton G, Chang WN, Dabney KW, Miller F. Surgical correction of scoliosis in pediatric patients with cerebral palsy using the unit rod instrumentation. Spine. 2008;33(10):1133–1140. - PubMed
-
- Samdani AF, Torre-Healy A, Asghar J, Herlich AM, Betz RR. Strategies to reduce blood loss during posterior spinal fusion for neuromuscular scoliosis: a review of current techniques and experience with a unique bipolar electrocautery device. Surg Technol Internat. 2008;17:243–248. - PubMed
-
- Mohamad F, Parent S, Pawelek J. Perioperative complications after surgical correction in neuromuscular scoliosis. J Pediatr Orthop. 2007;27(4):392–397. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous