

Is the scale up of malaria intervention coverage also achieving equity?
- PMID: 20027289
- PMCID: PMC2791860
- DOI: 10.1371/journal.pone.0008409
Is the scale up of malaria intervention coverage also achieving equity?
Abstract
Background and methods: Malaria in Africa is most severe in young children and pregnant women, particularly in rural and poor households. In many countries, malaria intervention coverage rates have increased as a result of scale up; but this may mask limited coverage in these highest-risk populations. Reports were reviewed from nationally representative surveys in African malaria-endemic countries from 2006 through 2008 to understand how reported intervention coverage rates reflect access by the most at-risk populations.
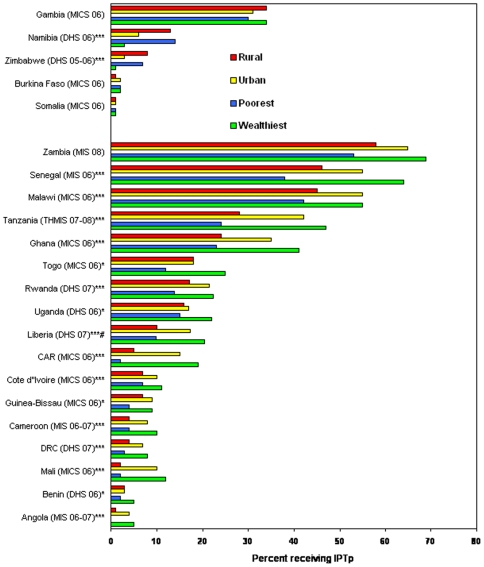
Results: Reports were available from 27 Demographic and Health Surveys (DHSs), Multiple Indicator Cluster Surveys (MICSs), and Malaria Indicator Surveys (MISs) during this interval with data on household intervention coverage by urban or rural setting, wealth quintile, and sex. Household ownership of insecticide-treated mosquito nets (ITNs) varied from 5% to greater than 60%, and was equitable by urban/rural and wealth quintile status among 13 (52%) of 25 countries. Malaria treatment rates for febrile children under five years of age varied from less than 10% to greater than 70%, and while equitable coverage was achieved in 8 (30%) of 27 countries, rates were generally higher in urban and richest quintile households. Use of intermittent preventive treatment in pregnant women varied from 2% to more than 60%, and again tended to be higher in urban and richest quintile households. Across all countries, there were no significant male/female inequalities seen for children sleeping under ITNs or receiving antimalarial treatment for febrile illness. Parasitemia and anemia rates from eight national surveys showed predominance in poor and rural populations.
Conclusions/significance: Recent efforts to scale up malaria intervention coverage have achieved equity in some countries (especially with ITNs), but delivery methods in other countries are not addressing the most at-risk populations. As countries seek universal malaria intervention coverage, their delivery systems must reach the rural and poor populations; this is not a small task, but it has been achieved in some countries.
Conflict of interest statement
Figures






Similar articles
-
Malaria indicator survey 2007, Ethiopia: coverage and use of major malaria prevention and control interventions.Malar J. 2010 Feb 24;9:58. doi: 10.1186/1475-2875-9-58. Malar J. 2010. PMID: 20178654 Free PMC article.
-
Socio-economic and demographic disparities in ownership and use of insecticide-treated bed nets for preventing malaria among rural reproductive-aged women in northern Ghana.PLoS One. 2019 Jan 29;14(1):e0211365. doi: 10.1371/journal.pone.0211365. eCollection 2019. PLoS One. 2019. PMID: 30695044 Free PMC article.
-
Estimating the number of insecticide-treated nets required by African households to reach continent-wide malaria coverage targets.JAMA. 2007 May 23;297(20):2241-50. doi: 10.1001/jama.297.20.2241. JAMA. 2007. PMID: 17519414 Review.
-
Coverage of intermittent preventive treatment and insecticide-treated nets for the control of malaria during pregnancy in sub-Saharan Africa: a synthesis and meta-analysis of national survey data, 2009-11.Lancet Infect Dis. 2013 Dec;13(12):1029-42. doi: 10.1016/S1473-3099(13)70199-3. Epub 2013 Sep 18. Lancet Infect Dis. 2013. PMID: 24054085 Review.
-
Sustained high coverage of insecticide-treated bednets through combined Catch-up and Keep-up strategies.Trop Med Int Health. 2007 Jul;12(7):815-22. doi: 10.1111/j.1365-3156.2007.01862.x. Trop Med Int Health. 2007. PMID: 17596247
Cited by
-
Scaling up impact of malaria control programmes: a tale of events in Sub-Saharan Africa and People's Republic of China.Infect Dis Poverty. 2012 Nov 1;1(1):7. doi: 10.1186/2049-9957-1-7. Infect Dis Poverty. 2012. PMID: 23849299 Free PMC article.
-
The pitfalls of scaling up evidence-based interventions in health.Glob Health Action. 2019;12(1):1670449. doi: 10.1080/16549716.2019.1670449. Glob Health Action. 2019. PMID: 31575331 Free PMC article.
-
Coverage of malaria protection in pregnant women in sub-Saharan Africa: a synthesis and analysis of national survey data.Lancet Infect Dis. 2011 Mar;11(3):190-207. doi: 10.1016/S1473-3099(10)70295-4. Epub 2011 Jan 26. Lancet Infect Dis. 2011. PMID: 21273130 Free PMC article.
-
Prevalence of malaria infection in pregnant women compared with children for tracking malaria transmission in sub-Saharan Africa: a systematic review and meta-analysis.Lancet Glob Health. 2015 Oct;3(10):e617-28. doi: 10.1016/S2214-109X(15)00049-2. Epub 2015 Aug 19. Lancet Glob Health. 2015. PMID: 26296450 Free PMC article.
-
Inequities in the use of sulphadoxine-pyrimethamine for malaria prophylaxis during pregnancy in Nigeria.Malawi Med J. 2020 Mar;32(1):45-51. doi: 10.4314/mmj.v32i1.9. Malawi Med J. 2020. PMID: 32733659 Free PMC article.
References
-
- Hay SI, Guerra CA, Gething PW, Patil AP, Tatem AJ, et al. A world malaria map: Plasmodium falciparum endemicity in 2007. PLoS Med. 2009;6:e1000048. doi: 10.1371/journal.pmed.1000048. - DOI - PMC - PubMed
-
- Gwatkin DR, Guillot M, Heuveline P. The burden of disease among the global poor. Lancet. 1999;354:586–589. - PubMed
-
- Greenwood BM, Bradley AK, Greenwood AM, Byass P, Jammeh K, et al. Mortality and morbidity from malaria among children in a rural area of The Gambia, West Africa. Trans R Soc Trop Med Hyg. 1987;81:478–486. - PubMed
-
- Binka FN, Morris SS, Ross DA, Arthur P, Aryeetey ME. Patterns of malaria morbidity and mortality in children in northern Ghana. Trans R Soc Trop Med Hyg. 1994;88:381–385. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
