

MRI versus 64-row MDCT for diagnosis of hepatocellular carcinoma
- PMID: 20027676
- PMCID: PMC2797660
- DOI: 10.3748/wjg.15.6044
MRI versus 64-row MDCT for diagnosis of hepatocellular carcinoma
Abstract
Aim: To compare the diagnostic capability of multidetector computed tomography (MDCT) and magnetic resonance imaging (MRI) for the detection of hepatocellular carcinoma (HCC) tumour nodules and their effect on patient management.
Methods: A total of 28 patients (25 male, 3 female, mean age 67 +/- 10.8 years) with biopsy-proven HCC were investigated with 64-row MDCT (slice 3 mm native, arterial and portal-venous phase, 120 mL Iomeprol, 4 mL/s, delay by bolus trigger) and MRI (T1fs fl2d TE/TR 2.72/129 ms, T2tse TE/TR 102/4000 ms, 5-phase dynamic contrast-enhanced T1fs fl3d TE/TR 1.56/4.6, Gadolinium-DTPA, slice 4 mm). Consensus reading of both modalities was used as reference. Tumour nodules were analyzed with respect to number, size, and location.
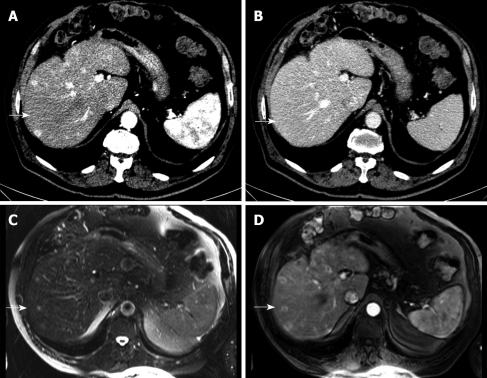
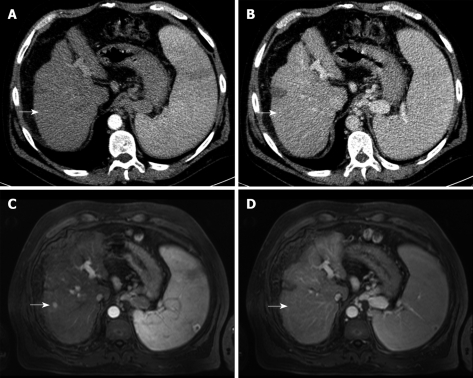
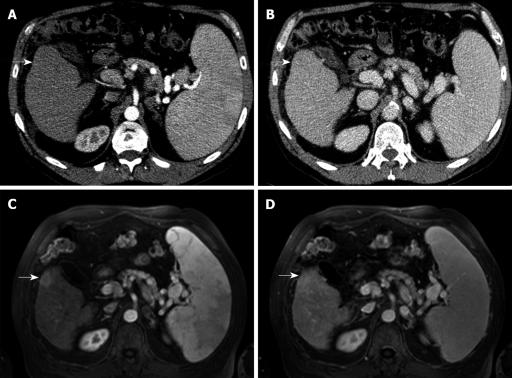
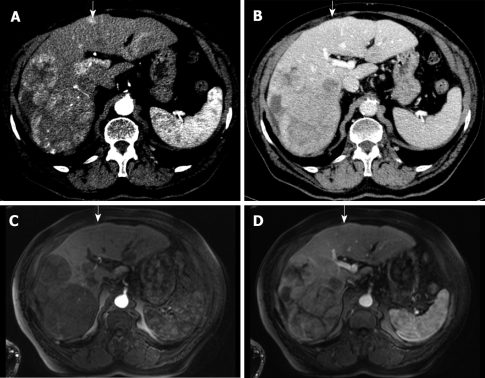
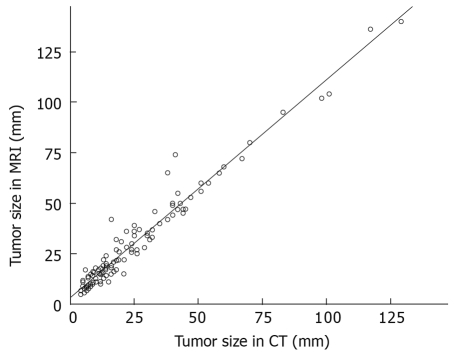
Results: In total, 162 tumour nodules were detected by consensus reading. MRI detected significantly more tumour nodules (159 vs 123, P < 0.001) compared to MDCT, with the best sensitivity for early arterial phase MRI. False-negative CT findings included nodules < or = 5 mm ( n = 5), < or = 10 mm ( n = 17), < or = 15 mm ( n = 12 ), < or = 20 mm ( n = 4 ), and 1 nodule > 20 mm. MRI missed 2 nodules < or = 10 mm and 1 nodule < or = 15 mm. On MRI, nodule diameters were greater than on CT (29.2 +/- 25.1 mm, range 5-140 mm vs 24.1 +/- 22.7 mm, range 4-129 mm, P < 0.005). In 2 patients, MDCT showed only unilobar tumour spread, whereas MRI revealed additional nodules in the contralateral lobe. Detection of these nodules could have changed the therapeutic strategy.
Conclusion: Contrast-enhanced MRI is superior to 64-row MDCT for the detection of HCC nodules. Patients should be allocated to interventional or operative treatment according to a dedicated MRI-protocol.
Figures
Similar articles
-
MDCT versus MRI assessment of tumor response after transarterial chemoembolization for the treatment of hepatocellular carcinoma.Cardiovasc Intervent Radiol. 2010 Jun;33(3):532-40. doi: 10.1007/s00270-009-9728-y. Epub 2009 Oct 22. Cardiovasc Intervent Radiol. 2010. PMID: 19847482
-
Small (<or=3 cm) hepatocellular carcinoma in cirrhosis: the role of double contrast agents in MR imaging vs. multidetector-row CT.Radiol Med. 2009 Dec;114(8):1239-66. doi: 10.1007/s11547-009-0439-x. Epub 2009 Aug 20. Radiol Med. 2009. PMID: 19697104
-
Efficacy of double arterial phase dynamic magnetic resonance imaging with the sensitivity encoding technique versus dynamic multidetector-row helical computed tomography for detecting hypervascular hepatocellular carcinoma.Jpn J Radiol. 2009 Jul;27(6):229-36. doi: 10.1007/s11604-009-0327-2. Epub 2009 Jul 22. Jpn J Radiol. 2009. PMID: 19626408
-
[Multiple-phase spiral computerized tomography of small hepatocellular carcinoma: technique optimization and diagnostic yield].Radiol Med. 1999 Jul-Aug;98(1-2):53-64. Radiol Med. 1999. PMID: 10566297 Review. Italian.
-
Ultrasonography, computed tomography and magnetic resonance imaging of hepatocellular carcinoma: toward improved treatment decisions.Oncology. 2011;81 Suppl 1:86-99. doi: 10.1159/000333267. Epub 2011 Dec 22. Oncology. 2011. PMID: 22212941 Review.
Cited by
-
MRI of hepatocellular carcinoma: an update of current practices.Diagn Interv Radiol. 2014 May-Jun;20(3):209-21. doi: 10.5152/dir.2014.13370. Diagn Interv Radiol. 2014. PMID: 24808419 Free PMC article. Review.
-
Considerations regarding current diagnosis and prognosis of hepatocellular carcinoma.J Med Life. 2015 Apr-Jun;8(2):120-8. J Med Life. 2015. PMID: 25866565 Free PMC article. Review.
-
Quantum iterative reconstruction on a photon-counting detector CT improves the quality of hepatocellular carcinoma imaging.Cancer Imaging. 2023 Jul 21;23(1):69. doi: 10.1186/s40644-023-00592-5. Cancer Imaging. 2023. PMID: 37480062 Free PMC article.
-
Does a combined CT and MRI protocol enhance the diagnostic efficacy of LI-RADS in the categorization of hepatic observations? A prospective comparative study.Eur Radiol. 2018 Jun;28(6):2592-2603. doi: 10.1007/s00330-017-5232-y. Epub 2018 Jan 24. Eur Radiol. 2018. PMID: 29368164
-
Liver imaging reporting and data system (LI-RADS) v2018: comparison between computed tomography and gadoxetic acid-enhanced magnetic resonance imaging.Jpn J Radiol. 2019 Sep;37(9):651-659. doi: 10.1007/s11604-019-00855-x. Epub 2019 Jul 18. Jpn J Radiol. 2019. PMID: 31321619
References
-
- Parkin DM, Bray F, Ferlay J, Pisani P. Estimating the world cancer burden: Globocan 2000. Int J Cancer. 2001;94:153–156. - PubMed
-
- Liu Q, Song Y, Zhou Y, Qiao L. A useful agent for chemoprevention of hepatocellular carcinoma? Cancer Biol Ther. 2006;5:1674–1676. - PubMed
-
- Bruix J, Barrera JM, Calvet X, Ercilla G, Costa J, Sanchez-Tapias JM, Ventura M, Vall M, Bruguera M, Bru C. Prevalence of antibodies to hepatitis C virus in Spanish patients with hepatocellular carcinoma and hepatic cirrhosis. Lancet. 1989;2:1004–1006. - PubMed
-
- El-Serag HB, Mason AC. Risk factors for the rising rates of primary liver cancer in the United States. Arch Intern Med. 2000;160:3227–3230. - PubMed
-
- Nair S, Shiv Kumar K, Thuluvath PJ. Mortality from hepatocellular and biliary cancers: changing epidemiological trends. Am J Gastroenterol. 2002;97:167–171. - PubMed
