

Assessment of in-stent restenosis using 64-MDCT: analysis of the CORE-64 Multicenter International Trial
- PMID: 20028909
- PMCID: PMC3294284
- DOI: 10.2214/AJR.09.2652
Assessment of in-stent restenosis using 64-MDCT: analysis of the CORE-64 Multicenter International Trial
Abstract
Objective: Evaluations of stents by MDCT from studies performed at single centers have yielded variable results with a high proportion of unassessable stents. The purpose of this study was to evaluate the accuracy of 64-MDCT angiography (MDCTA) in identifying in-stent restenosis in a multicenter trial.
Materials and methods: The Coronary Evaluation Using Multidetector Spiral Computed Tomography Angiography Using 64 Detectors (CORE-64) Multicenter Trial and Registry evaluated the accuracy of 64-MDCTA in assessing 405 patients referred for coronary angiography. A total of 75 stents in 52 patients were assessed: 48 of 75 stents (64%) in 36 of 52 patients (69%) could be evaluated. The prevalence of in-stent restenosis by quantitative coronary angiography (QCA) in this subgroup was 23% (17/75). Eighty percent of the stents were <or=3.0 mm in diameter.
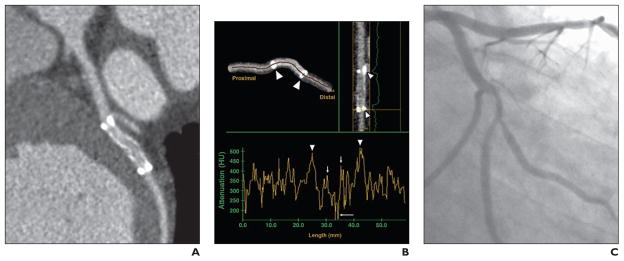
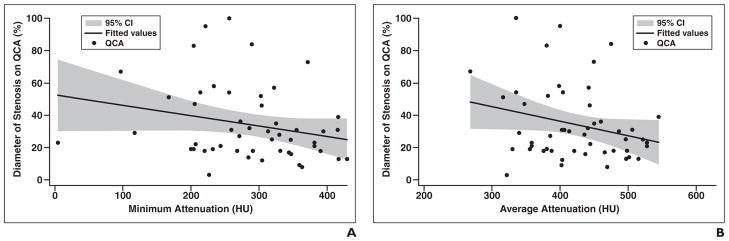
Results: The overall sensitivity, specificity, positive predictive value, and negative predictive value to detect 50% in-stent stenosis visually using MDCT compared with QCA was 33.3%, 91.7%, 57.1%, and 80.5%, respectively, with an overall accuracy of 77.1% for the 48 assessable stents. The ability to evaluate stents on MDCTA varied by stent type: Thick-strut stents such as Bx Velocity were assessable in 50% of the cases; Cypher, 62.5% of the cases; and thinner-strut stents such as Taxus, 75% of the cases. We performed quantitative assessment of in-stent contrast attenuation in Hounsfield units and correlated that value with the quantitative percentage of stenosis by QCA. The correlation coefficient between the average attenuation decrease and >or=50% stenosis by QCA was 0.25 (p=0.073). Quantitative assessment failed to improve the accuracy of MDCT over qualitative assessment.
Conclusion: The results of our study showed that 64-MDCT has poor ability to detect in-stent restenosis in small-diameter stents. Evaluability and negative predictive value were better in large-diameter stents. Thus, 64-MDCT may be appropriate for stent assessment in only selected patients.
Figures
References
-
- King SB, 3rd, Smith SC, Jr, Hirshfeld JW, Jr, et al. 2007 focused update of the ACC/AHA/SCAI 2005 guideline update for percutaneous coronary intervention: a report of the American College of Cardiology/American Heart Association Task Force on Practice guidelines. J Am Coll Cardiol. 2008;51:172–209. - PubMed
-
- Serruys PW, de Jaegere P, Kiemeneij F, et al. A comparison of balloon-expandable-stent implantation with balloon angioplasty in patients with coronary artery disease. Benestent Study Group. N Engl J Med. 1994;331:489–495. - PubMed
-
- Fischman DL, Leon MB, Baim DS, et al. A randomized comparison of coronary-stent placement and balloon angioplasty in the treatment of coronary artery disease. Stent Restenosis Study Investigators. N Engl J Med. 1994;331:496–501. - PubMed
-
- Serruys PW, Foley DP, Suttorp MJ, et al. A randomized comparison of the value of additional stenting after optimal balloon angioplasty for long coronary lesions: final results of the additional value of NIR stents for treatment of long coronary lesions (ADVANCE) study. J Am Coll Cardiol. 2002;39:393–399. - PubMed
-
- Stettler C, Wandel S, Allemann S, et al. Outcomes associated with drug-eluting and bare-metal stents: a collaborative network meta-analysis. Lancet. 2007;370:937–948. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
