

Review
doi: 10.4103/0301-4738.58470.
Current approach in the diagnosis and management of posterior uveitis
Affiliations
- PMID: 20029144
- PMCID: PMC2841371
- DOI: 10.4103/0301-4738.58470
Item in Clipboard
Review
Current approach in the diagnosis and management of posterior uveitis
Indian J Ophthalmol.
2010 Jan-Feb.
Abstract
Posterior uveitic entities are varied entities that are infective or non-infective in etiology. They can affect the adjacent structures such as the retina, vitreous, optic nerve head and retinal blood vessels. Thorough clinical evaluation gives a clue to the diagnosis while ancillary investigations and laboratory tests assist in confirming the diagnosis. Newer evolving techniques in the investigations and management have increased the diagnostic yield. In case of diagnostic dilemma, intraocular fluid evaluation for polymerase chain testing for the genome and antibody testing against the causative agent provide greater diagnostic ability.
Conflict of interest statement
Figures
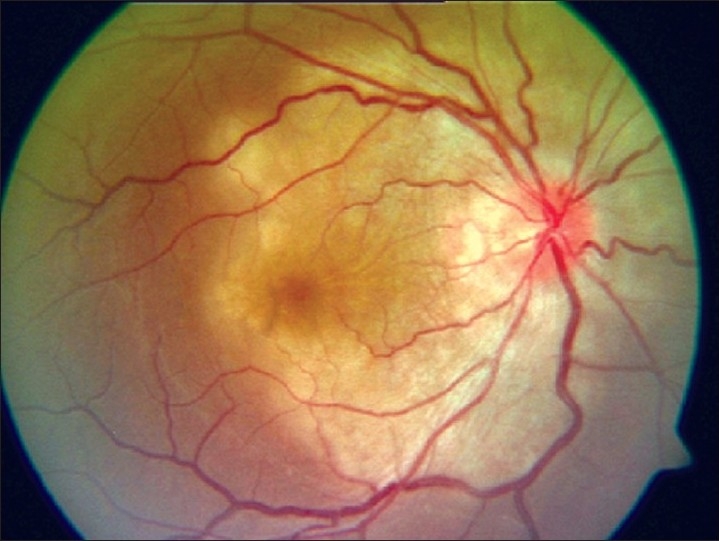
Fundus picture showing a typical punched-out macular scar of a healed congenital toxoplasmosis
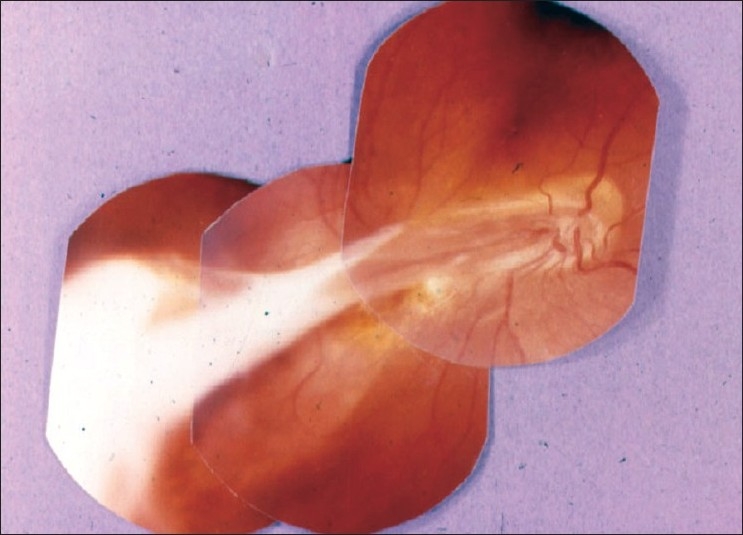
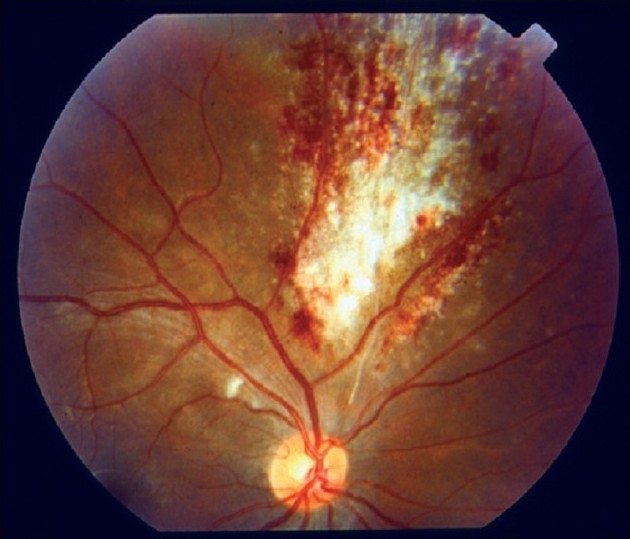
Fundus picture showing a typical “headlight in the fog appearance” in a patient with acquired toxoplasmosis
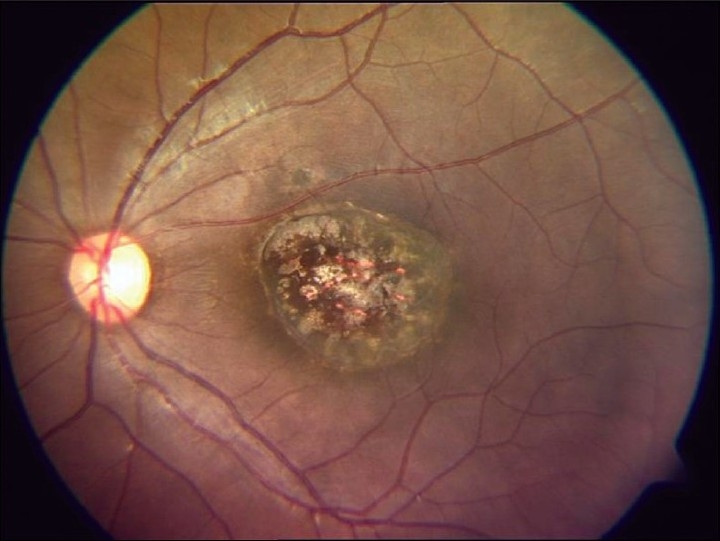
Fundus picture showing a toxocara granuloma
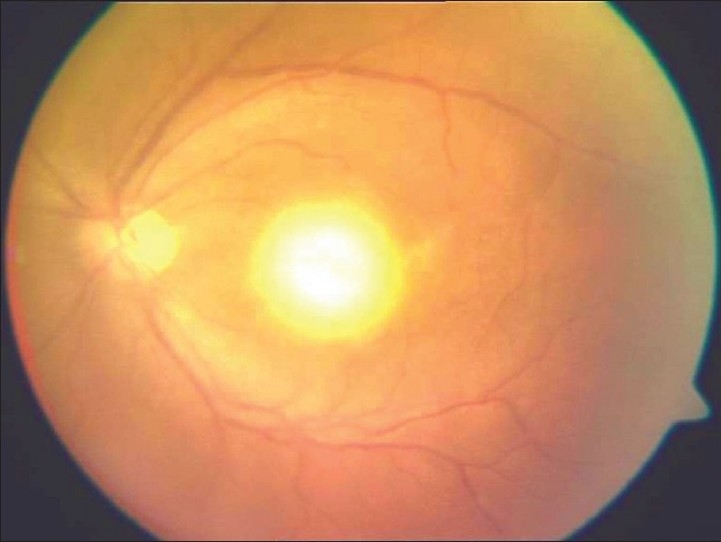
Fundus picture showing a tuberculous subretinal abscess

Fundus picture showing the classical “cracked mud appearance” in progressive outer retinal necrosis
Fundus picture showing a typical “pizza pie appearance” in a patient with cytomegalovirus retinitis
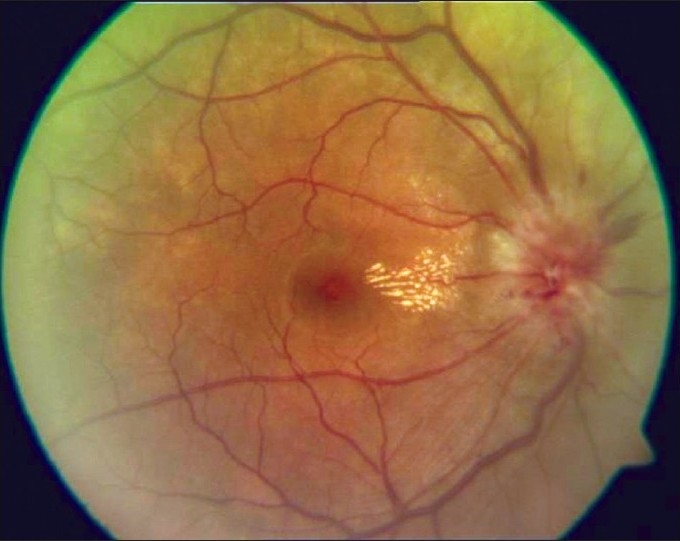
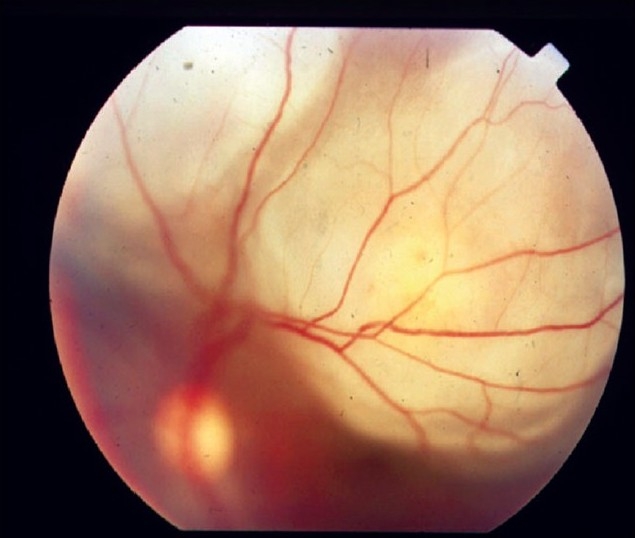
Fundus picture showing disc edema and macular exudates characteristic of a neuroretinitis

Fundus picture showing placoid lesions of acute posterior multifocal placoid pigment epitheliopathy
Fundus picture showing active geographic helicoid peripapillary choroidopathy
Comment in
-
Autofluorescence in posterior uveitis.Indian J Ophthalmol. 2010 Sep-Oct;58(5):443. doi: 10.4103/0301-4738.67040. Indian J Ophthalmol. 2010. PMID: 20689208 Free PMC article. No abstract available.
Similar articles
-
[Ocular manifestations of syphilitic uveoretinitis in patients co-infected with human immunodeficiency virus].Zhonghua Yan Ke Za Zhi. 2015 Oct;51(10):739-45. Zhonghua Yan Ke Za Zhi. 2015. PMID: 26693768 Chinese.
-
Optical Coherence Tomography Findings in Infectious Posterior Uveitis.Ocul Immunol Inflamm. 2022 Apr 3;30(3):652-663. doi: 10.1080/09273948.2022.2032197. Epub 2022 Feb 28. Ocul Immunol Inflamm. 2022. PMID: 35226572 Review.
-
Retinal meteor.Indian J Ophthalmol. 2017 Sep;65(9):879-881. doi: 10.4103/ijo.IJO_68_17. Indian J Ophthalmol. 2017. PMID: 28905838 Free PMC article.
-
Optic Disc Neovascularization in Tubercular Serpiginous-Like Choroiditis.Ocul Immunol Inflamm. 2020 May 18;28(4):676-678. doi: 10.1080/09273948.2019.1622736. Epub 2019 Aug 12. Ocul Immunol Inflamm. 2020. PMID: 31403829
-
Current approach in diagnosis and management of anterior uveitis.Indian J Ophthalmol. 2010 Jan-Feb;58(1):11-9. doi: 10.4103/0301-4738.58468. Indian J Ophthalmol. 2010. PMID: 20029142 Free PMC article. Review.
Cited by
-
Bilateral choroidal tuberculoma in miliary tuberculosis - report of a case.J Ophthalmic Inflamm Infect. 2015 Feb 13;5:4. doi: 10.1186/s12348-014-0032-x. eCollection 2015. J Ophthalmic Inflamm Infect. 2015. PMID: 25861395 Free PMC article.
-
Fluorescein and indocyanine-green angiography in ocular syphilis: an exploratory study.Graefes Arch Clin Exp Ophthalmol. 2012 May;250(5):721-30. doi: 10.1007/s00417-011-1893-4. Epub 2011 Dec 25. Graefes Arch Clin Exp Ophthalmol. 2012. PMID: 22198216
-
Deep Learning-Based Detection of Early Renal Function Impairment Using Retinal Fundus Images: Model Development and Validation.JMIR Med Inform. 2020 Nov 26;8(11):e23472. doi: 10.2196/23472. JMIR Med Inform. 2020. PMID: 33139242 Free PMC article.
-
Role of multicolour imaging in post-fever retinitis involving posterior pole.Int Ophthalmol. 2021 Nov;41(11):3797-3804. doi: 10.1007/s10792-021-01951-6. Epub 2021 Jul 14. Int Ophthalmol. 2021. PMID: 34263386
-
Galactic vision: asteroid hyalosis in vitreous with moonlit optic disc.BMJ Case Rep. 2024 May 6;17(5):e260387. doi: 10.1136/bcr-2024-260387. BMJ Case Rep. 2024. PMID: 38719250 No abstract available.
References
-
- Foster CS, Vittale AT, editors. Diagnosis and treatment of uveitis. Philadelphia: WB Saunders Company; 2002. pp. 264–72.pp. 315–32.pp. 710–25.pp. 731–812.
-
- Bonfioli AA, Orefice F. Toxoplasmosis. Semin Ophthalmol. 2005;20:129–41. - PubMed
-
- Palanisamy M, Madhavan B, Balasundaram MB, Andavar R, Venkatapathy N. Outbreak of ocular toxoplasmosis in Coimbatore, India. Indian J Ophthalmol. 2006;54:129–31. - PubMed
-
- Kraushar MF, Gluck SB, Pass S. Toxoplasmic retinochoroiditis presenting as serous detachment of the macula. Ann Ophthalmol. 1979;11:1513–4. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
