

Bundled care for septic shock: an analysis of clinical trials
- PMID: 20029343
- PMCID: PMC3383776
- DOI: 10.1097/CCM.0b013e3181cb0ddf
Bundled care for septic shock: an analysis of clinical trials
Abstract
Context: Sepsis bundles have been developed to improve patient outcomes by combining component therapies. Valid bundles require effective components with additive benefits. Proponents encourage evaluation of bundles, both as a whole and based on the performance of each component.
Objective: Assess the association between outcome and the utilization of component therapies in studies of sepsis bundles.
Data source: Database searches (January 1980 to July 2008) of PubMed, Embase, and the Cochrane Library, using the terms sepsis, bundles, guidelines, and early goal directed therapy.
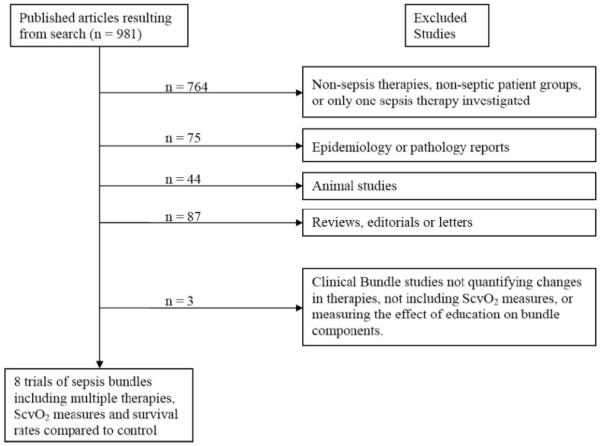
Data extraction: Inclusion required comparison of septic adults who received bundled care vs. nonprotocolized care. Survival and use rates for individual interventions were abstracted.
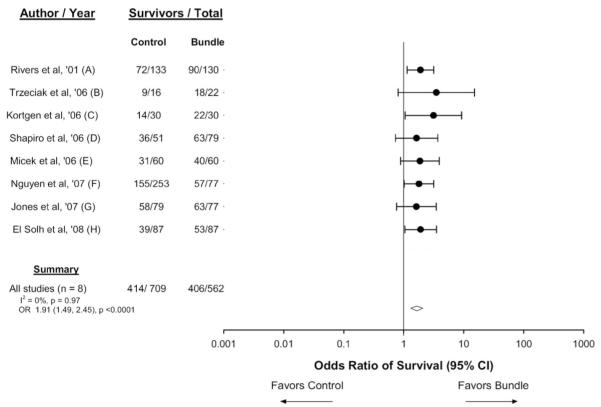
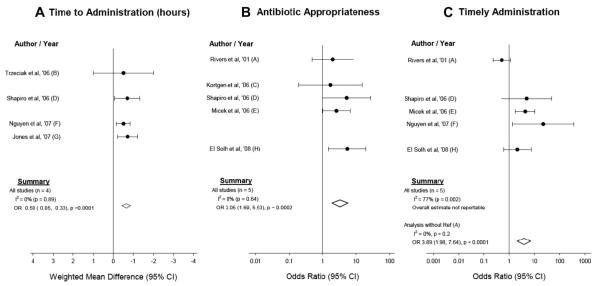
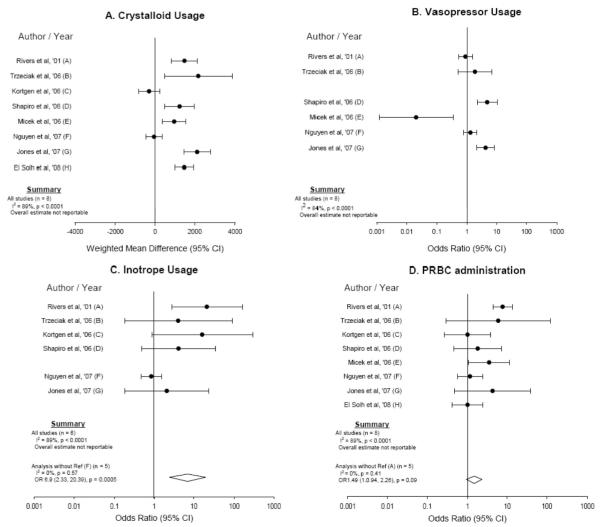
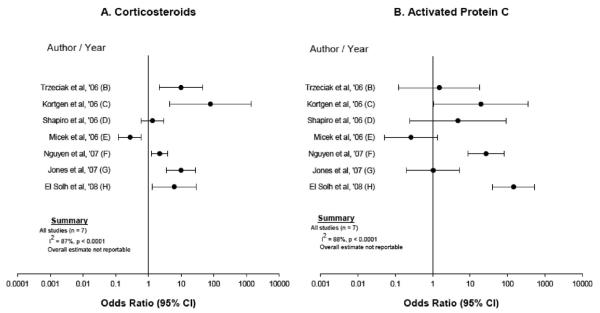
Main results: Eight unblinded trials, one randomized and seven with historical controls, were identified. Sepsis bundles were associated with a consistent (I2 = 0%, p = .87) and significant increase in survival (odds ratio, 1.91; 95% confidence interval, 1.49-2.45; p < .0001). For all studies reporting such data, there were consistent (I2 = 0%, p > or = .64) decreases in time to antibiotics, and increases in the appropriateness of antibiotics (p < or = .0002 for both). In contrast, significant heterogeneity was seen across trials for all other treatments (antibiotic use within a specified time period; administration of fluids, vasopressors, inotropes, and packed red blood cells titrated to hemodynamic goals; corticosteroids and human recombinant activated protein C use) (all I2 > or = 67%, p < .002). Except for antibiotics, sepsis bundle components are still being investigated for efficacy in randomized controlled trials.
Conclusion: Bundle use was associated with consistent and significant improvement in survival and antibiotic use. Use of other bundle components changed heterogeneously across studies, making their impact on survival uncertain. However, this analysis should be interpreted cautiously as these studies were unblinded, and only one was randomized.
Figures
Comment in
-
A magic bullet for sepsis: getting back to the basics.Crit Care Med. 2010 Feb;38(2):733-4. doi: 10.1097/CCM.0b013e3181c895a8. Crit Care Med. 2010. PMID: 20083953 No abstract available.
References
-
- [Accessed September 2, 2009];Raising the bar with bundles: Improving the quality of care by improving the work environment. Joint Commission Perspectives on Patient Safety. 2006 Apr;6:5–6. Available at: http://www.ingentaconnect.com/content/jcaho/jcpps/2006/00000006/00000004....
-
- Pronovost PJ, Berenholtz SM, Ngo K, et al. Developing and testing quality indicators in the intensive care unit. J Crit Care. 2003;18:145–155. - PubMed
-
- Pronovost P, Needham D, Berenholtz S, et al. An intervention to decrease catheter-related blood stream infections in the ICU. N Engl J Med. 2006;355:2725–2732. - PubMed
-
- Fullbrook P, Mooney S. Care bundles in critical care: A practical approach to evidence-based practice. Nurs Crit Care. 2003;8:249–255. - PubMed
-
- Centers for Medicare and Medicaid Services [Accessed May 26th, 2009];8th Scope of Work (version 080105-1) Available at http://www.cms.hhs.gov/QualityImprovementOrgs/Downloads/8thSOW.pdf.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
