

Acute effects of gastric bypass versus gastric restrictive surgery on beta-cell function and insulinotropic hormones in severely obese patients with type 2 diabetes
- PMID: 20029383
- PMCID: PMC2838991
- DOI: 10.1038/ijo.2009.254
Acute effects of gastric bypass versus gastric restrictive surgery on beta-cell function and insulinotropic hormones in severely obese patients with type 2 diabetes
Abstract
Context: Hyperglycemia resolves quickly after bariatric surgery, but the underlying mechanism and the most effective type of surgery remains unclear.
Objective: To examine glucose metabolism and beta-cell function in patients with type 2 diabetes mellitus (T2DM) after two types of bariatric intervention; Roux-en-Y gastric bypass (RYGB) and gastric restrictive (GR) surgery.
Design: Prospective, nonrandomized, repeated-measures, 4-week, longitudinal clinical trial.
Patients: In all, 16 T2DM patients (9 males and 7 females, 52+/-14 years, 47+/-9 kg m(-2), HbA1c 7.2+/-1.1%) undergoing either RYGB (N=9) or GR (N=7) surgery.
Outcome measures: Glucose, insulin secretion, insulin sensitivity at baseline, and 1 and 4 weeks post-surgery, using hyperglycemic clamps and C-peptide modeling kinetics; glucose, insulin secretion and gut-peptide responses to mixed meal tolerance test (MMTT) at baseline and 4 weeks post-surgery.
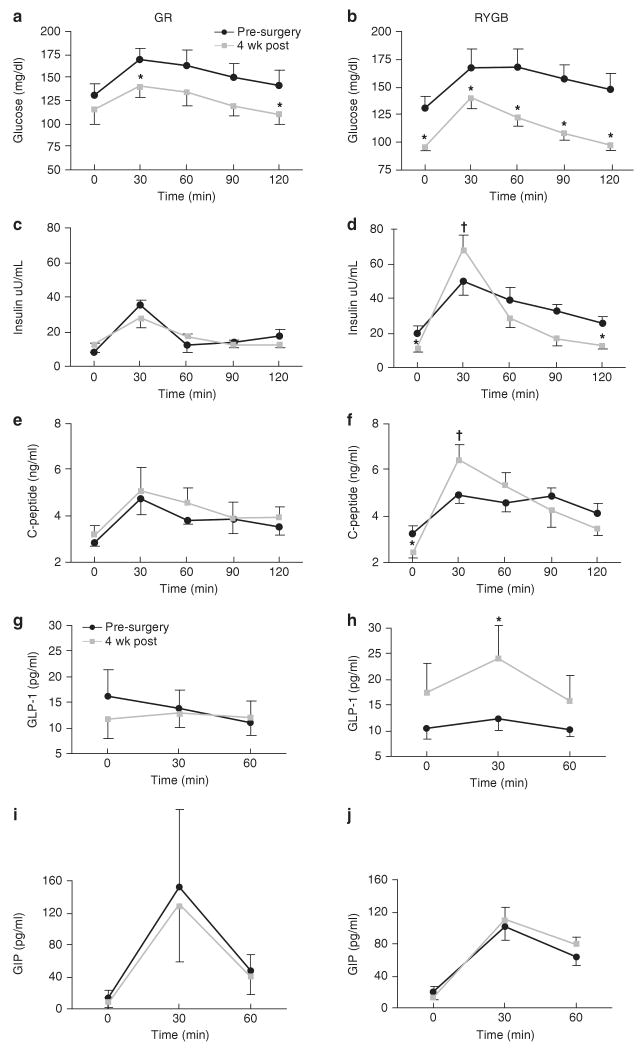
Results: At 1 week post-surgery, both groups experienced a similar weight loss and reduction in fasting glucose (P<0.01). However, insulin sensitivity increased only after RYGB, (P<0.05). At 4 weeks post-surgery, weight loss remained similar for both groups, but fasting glucose was normalized only after RYGB (95+/-3 mg 100 ml(-1)). Insulin sensitivity improved after RYGB (P<0.01) and did not change with GR, whereas the disposition index remained unchanged after RYGB and increased 30% after GR (P=0.10). The MMTT elicited a robust increase in insulin secretion, glucagon-like peptide-1 (GLP-1) levels and beta-cell sensitivity to glucose only after RYGB (P<0.05).
Conclusion: RYGB provides a more rapid improvement in glucose regulation compared with GR. This improvement is accompanied by enhanced insulin sensitivity and beta-cell responsiveness to glucose, in part because of an incretin effect.
Conflict of interest statement
Figures
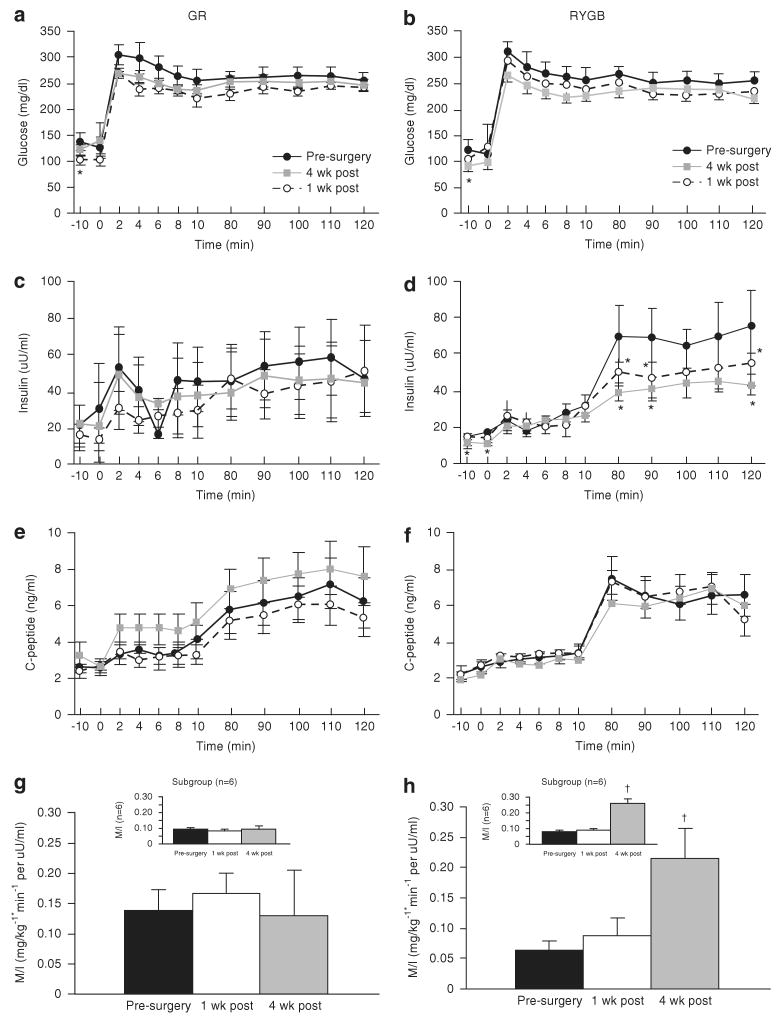
 ) after surgery. Insulin sensitivity was estimated from the M/I ratio by dividing the average glucose infusion (M value in mg kg−1 min−1) during the last 40 min of the clamp by the average plasma insulin concentration during that same interval (M/I) (g, h). Subgroup analysis of subjects with matched insulin sensitivity values are shown in panels for g, h. Values represent mean±s.e.m. *Significantly lower than the pre-surgery response, P<0.05. †Significantly greater than the pre-surgery response P<0.05.
) after surgery. Insulin sensitivity was estimated from the M/I ratio by dividing the average glucose infusion (M value in mg kg−1 min−1) during the last 40 min of the clamp by the average plasma insulin concentration during that same interval (M/I) (g, h). Subgroup analysis of subjects with matched insulin sensitivity values are shown in panels for g, h. Values represent mean±s.e.m. *Significantly lower than the pre-surgery response, P<0.05. †Significantly greater than the pre-surgery response P<0.05.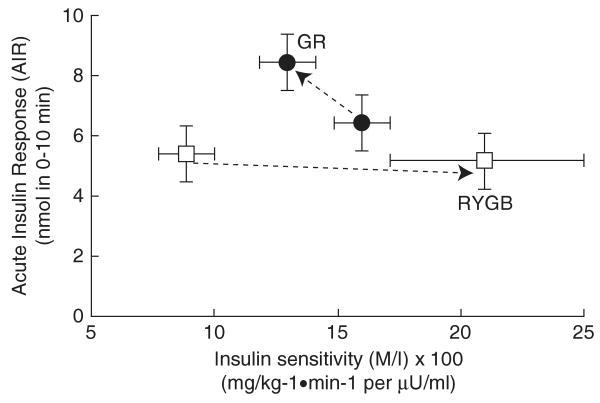
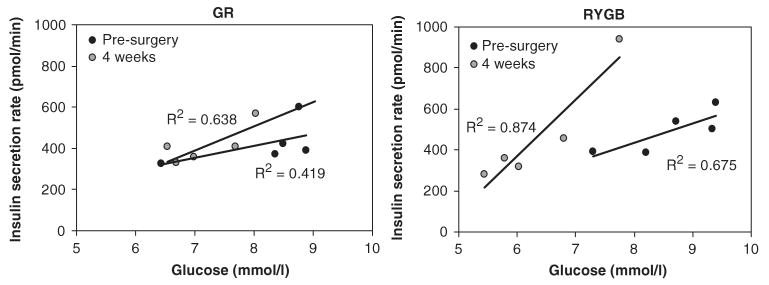
 ). The values of the slopes are indicated in Table 1. Comparison between slopes for RYGB (pre-surgery versus 4 weeks) was statistically different P<0.05. Comparison between pre-surgery slopes for RYGB versus GR was also statistically different P<0.05.
). The values of the slopes are indicated in Table 1. Comparison between slopes for RYGB (pre-surgery versus 4 weeks) was statistically different P<0.05. Comparison between pre-surgery slopes for RYGB versus GR was also statistically different P<0.05.Similar articles
-
Roux-en-Y gastric bypass and sleeve gastrectomy: mechanisms of diabetes remission and role of gut hormones.J Clin Endocrinol Metab. 2013 Nov;98(11):4391-9. doi: 10.1210/jc.2013-2538. Epub 2013 Sep 20. J Clin Endocrinol Metab. 2013. PMID: 24057293
-
Mechanisms of improved glycaemic control after Roux-en-Y gastric bypass.Dan Med J. 2015 Apr;62(4):B5057. Dan Med J. 2015. PMID: 25872541 Review.
-
Preserved Insulin Secretory Capacity and Weight Loss Are the Predominant Predictors of Glycemic Control in Patients With Type 2 Diabetes Randomized to Roux-en-Y Gastric Bypass.Diabetes. 2015 Sep;64(9):3104-10. doi: 10.2337/db14-1870. Epub 2015 Apr 21. Diabetes. 2015. PMID: 25901097 Free PMC article. Clinical Trial.
-
Gastrointestinal Hormones and β-Cell Function After Gastric Bypass and Sleeve Gastrectomy: A Randomized Controlled Trial (Oseberg).J Clin Endocrinol Metab. 2022 Jan 18;107(2):e756-e766. doi: 10.1210/clinem/dgab643. J Clin Endocrinol Metab. 2022. PMID: 34463768 Clinical Trial.
-
Mechanisms of early improvement/resolution of type 2 diabetes after bariatric surgery.Diabetes Metab. 2009 Dec;35(6 Pt 2):518-23. doi: 10.1016/S1262-3636(09)73459-7. Diabetes Metab. 2009. PMID: 20152737 Review.
Cited by
-
Very low-calorie diet mimics the early beneficial effect of Roux-en-Y gastric bypass on insulin sensitivity and β-cell Function in type 2 diabetic patients.Diabetes. 2013 Sep;62(9):3027-32. doi: 10.2337/db12-1762. Epub 2013 Apr 22. Diabetes. 2013. PMID: 23610060 Free PMC article. Clinical Trial.
-
Bariatric Surgery in Obese Patients With Type 1 Diabetes.Diabetes Care. 2016 Jun;39(6):941-8. doi: 10.2337/dc15-2732. Diabetes Care. 2016. PMID: 27222552 Free PMC article. Review.
-
A gut feeling to cure diabetes: potential mechanisms of diabetes remission after bariatric surgery.Diabetes Metab J. 2014 Dec;38(6):406-15. doi: 10.4093/dmj.2014.38.6.406. Diabetes Metab J. 2014. PMID: 25541603 Free PMC article. Review.
-
Type 2 diabetes, bariatric surgery and the risk of subsequent gestational diabetes.Obstet Med. 2011 Dec;4(4):171-3. doi: 10.1258/om.2011.110020. Epub 2011 Sep 15. Obstet Med. 2011. PMID: 27579120 Free PMC article.
-
The Leading Role of Peptide Tyrosine Tyrosine in Glycemic Control After Roux-en-Y Gastric Bypass in Rats.Obes Surg. 2020 Feb;30(2):697-706. doi: 10.1007/s11695-019-04239-y. Obes Surg. 2020. PMID: 31701411
References
-
- Defronzo RA. Pathogenesis of type 2 diabetes mellitus. Med Clin North Am. 2004;88:787–835. - PubMed
-
- Unger RH. Minireview: weapons of lean body mass destruction: the role of ectopic lipids in the metabolic syndrome. Endocrinology. 2003;144:5159–5165. - PubMed
-
- Gastaldelli A, Ferrannini E, Miyazaki Y, Matsuda M, Defronzo RA. Beta-cell dysfunction and glucose intolerance: results from the San Antonio metabolism (SAM) study. Diabetologia. 2004;47:31–39. - PubMed
-
- Polonsky KS, Gumbiner B, Ostrega D, Griver K, Tager H, Henry RR. Alterations in immunoreactive proinsulin and insulin clearance induced by weight loss in NIDDM. Diabetes. 1994;43:871–877. - PubMed
-
- Buchwald H, Avidor Y, Braunwald E, Jensen MD, Pories W, Fahrbach K, et al. Bariatric surgery: a systematic review and meta-analysis. JAMA. 2004;292:1724–1737. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
