

Fast track liver resection: the effect of a comprehensive care package and analgesia with single dose intrathecal morphine with gabapentin or continuous epidural analgesia
- PMID: 20029637
- PMCID: PMC2796218
- DOI: 10.1155/2009/271986
Fast track liver resection: the effect of a comprehensive care package and analgesia with single dose intrathecal morphine with gabapentin or continuous epidural analgesia
Abstract
Background: A comprehensive care package for patients undergoing hepatectomy was developed with the aim of minimal physiological disturbance in the peri-operative period. Peri-operative analgesia with few gastrointestinal effects and reduced requirement for intravenous (IV) fluid therapy was central to this plan.
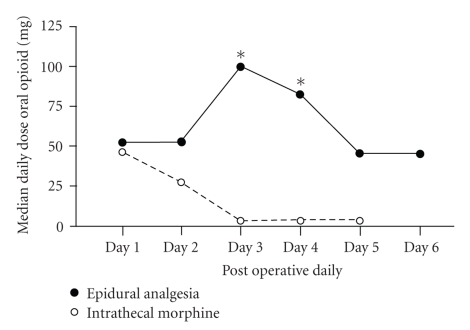
Methods: Data on 100 consecutive patients managed with continuous epidural infusion (n = 50; bupivicaine 0.125% and fentanyl 2 microg/mL at 0.1 mL/kg/hr) or intrathecal morphine (n = 50; 300 microg in combination with oral gabapentin 1200 mg preoperatively and 400 mg bd postoperatively) was compared.
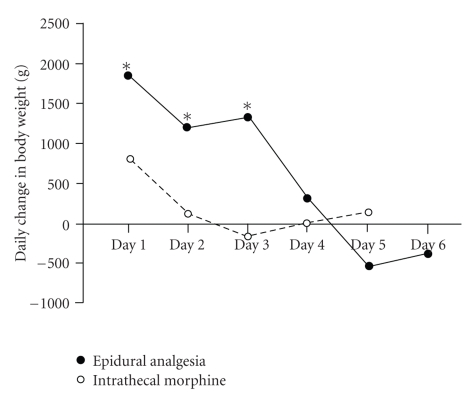
Results: The epidural and intrathecal morphine groups were equivalent in terms of patient demographics, procedures and complications. Patients receiving intrathecal morphine received less intra-operative IV fluids (median 1500 mL versus 2200 mL, P = .06), less postoperative IV fluids (median 1200 mL versus 4300 mL, P = .03) than patients receiving epidural infusion. Patients managed with intrathecal morphine established a normal dietary intake sooner (16 hours versus 20 hours, P = .05) and had shorter hospital stays than those managed with epidural infusions (4.7 +/- 0.9 days versus 6.8 +/- 1.2 days, P = .02).
Conclusions: Single dose intrathecal morphine is a safe and effective means of providing peri-operative analgesia. Patients managed with intrathecal morphine have reduced peri-operative physiological disturbance and return home within a few days of hepatic resection.
Figures
References
-
- Foster JH, Berman MM. Solid Liver Tumors. Major Problems in Clinical Surgery. Vol. 22. Philadelphia, Pa, USA: WB Saunders; 1977. - PubMed
-
- Capussotti L, Muratore A, Ferrero A, Massucco P, Ribero D, Polastri R. Randomized clinical trial of liver resection with and without hepatic pedicle clamping. British Journal of Surgery. 2006;93(6):685–689. - PubMed
-
- Dimick JB, Wainess RM, Cowan JA, Upchurch GR, Jr., Knol JA, Colletti LM. National trends in the use and outcomes of hepatic resection. Journal of the American College of Surgeons. 2004;199(1):31–38. - PubMed
-
- Lobo DN, Bostock KA, Neal KR, Perkins AC, Rowlands BJ, Allison SP. Effect of salt and water balance on recovery of gastrointestinal function after elective colonic resection: a randomised controlled trial. The Lancet. 2002;359(9320):1812–1818. - PubMed
LinkOut - more resources
Full Text Sources
Medical
