

Cardiopulmonary complications leading to premature deaths in adult patients with sickle cell disease
- PMID: 20029950
- PMCID: PMC3865703
- DOI: 10.1002/ajh.21569
Cardiopulmonary complications leading to premature deaths in adult patients with sickle cell disease
Abstract
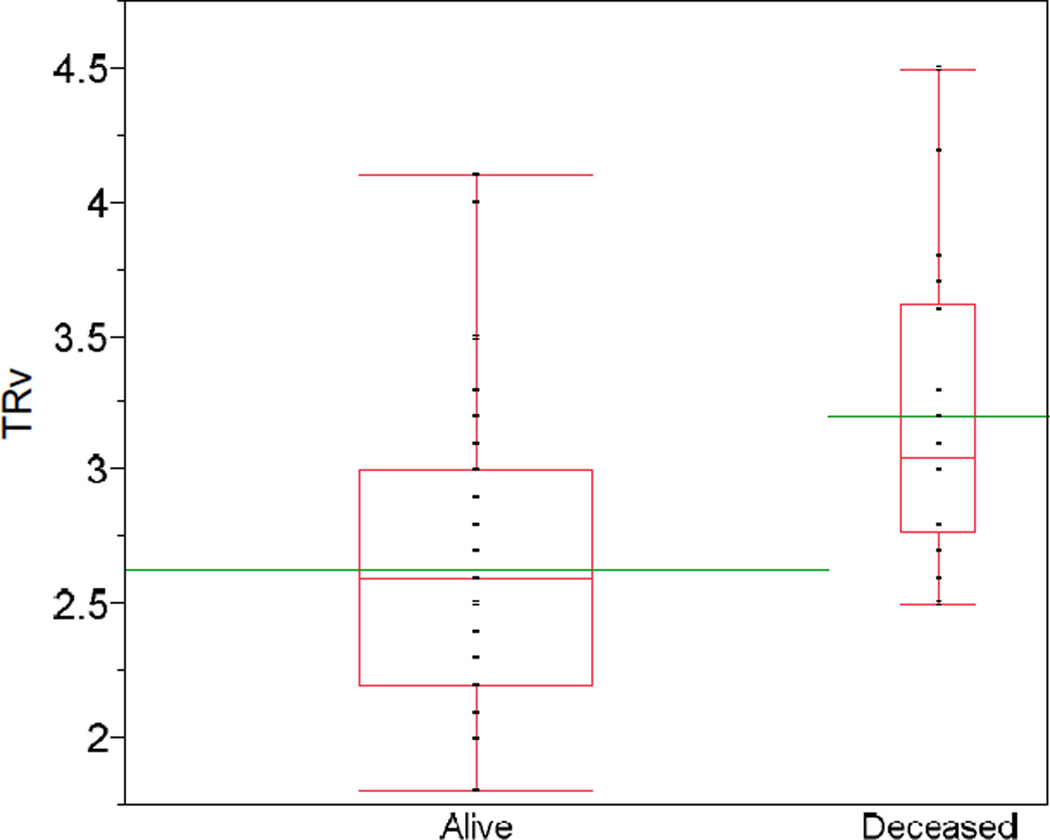
Sickle cell disease (SCD) is associated with early mortality. We sought to determine the incidence, cause, and risk factors for death in an adult population of patients with SCD. All patients aged >/=18 years seen at the Adult Sickle Cell Center at Duke University Medical Center between January 2000 and April 2005 were enrolled. Forty-three patients (21 males and 22 females) died during the study period. The median age of survival was 39 years for females (95% CI: 34-56), 40 years for males (95% CI: 34-48), and 40 years overall (95% CI: 35-48). Cardiac causes of death accounted for 25.6% (11/43 patients); pulmonary, 14.0% (six patients); other SCD related, 32.6% (14 patients); unknown, 14.0% (six patients); and others, 14.0% (six patients). Pulseless electrical activity arrest, pulmonary emboli, multiorgan failure, and stroke were the most frequent causes of death. Among the deceased patients, the most common premorbid conditions were cardiopulmonary: acute chest syndrome/pneumonia (58.1%), Pulmonary hypertension (pHTN; 41.9%), systemic HTN (25.6%), congestive heart failure (25.6%), myocardial infarction (20.9%), and arrhythmias (14.0%). Tricuspid regurgitant jet velocity was significantly higher (3.1 m/sec vs. 2.6 m/sec, P < 0.001) and hemoglobin significantly lower (8.3 g/dL vs. 9.2 g/dL, P < 0.05) in deceased patients when compared with patients who lived, respectively. With improved preventive and therapeutic advances, including hydroxyurea therapy, acute complications such as infection are no longer the leading cause of death; instead, causes of death and premorbid conditions are shifting to chronic cardiopulmonary complications. Further, arrhythmia leading to premature death is under-recognized in SCD and warrants further investigation.
(c) 2009 Wiley-Liss, Inc.
Figures
References
-
- Diggs LM. Sickle cell disease: diagnosis, management, education and research. Mosby: St. Louis; 1973. pp. 189–229.
-
- Schultz WH, Ware RE. Malignancy in patients with sickle cell disease. Am J Hematol. 2003;74:249–253. - PubMed
-
- Castro O, Hoque M, Brown BD. Pulmonary hypertension in sickle cell disease: cardiac catheterization results and survival. Blood. 2003;101:1257–1261. - PubMed
-
- Leikin SL, Gallagher D, Kinney TR, Sloane D, Klug P, Rida W. Mortality in children and adolescents with sickle cell disease. Cooperative Study of Sickle Cell Disease. Pediatrics. 1989;84:500–508. - PubMed
-
- Powars DR, Chan LS, Hiti A, Ramicone E, Johnson C. Outcome of sickle cell anemia: a 4-decade observational study of 1056 patients. Medicine (Baltimore) 2005;84:363–376. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous