

C-reactive protein concentration and risk of coronary heart disease, stroke, and mortality: an individual participant meta-analysis
- PMID: 20031199
- PMCID: PMC3162187
- DOI: 10.1016/S0140-6736(09)61717-7
C-reactive protein concentration and risk of coronary heart disease, stroke, and mortality: an individual participant meta-analysis
Abstract
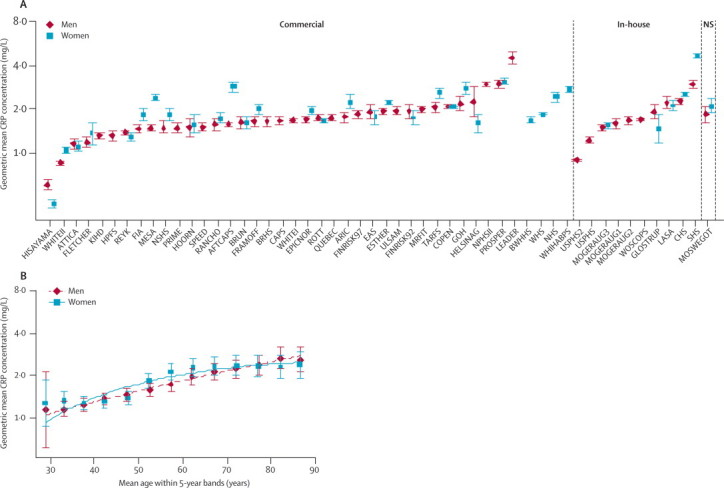
Background: Associations of C-reactive protein (CRP) concentration with risk of major diseases can best be assessed by long-term prospective follow-up of large numbers of people. We assessed the associations of CRP concentration with risk of vascular and non-vascular outcomes under different circumstances.
Methods: We meta-analysed individual records of 160 309 people without a history of vascular disease (ie, 1.31 million person-years at risk, 27 769 fatal or non-fatal disease outcomes) from 54 long-term prospective studies. Within-study regression analyses were adjusted for within-person variation in risk factor levels.
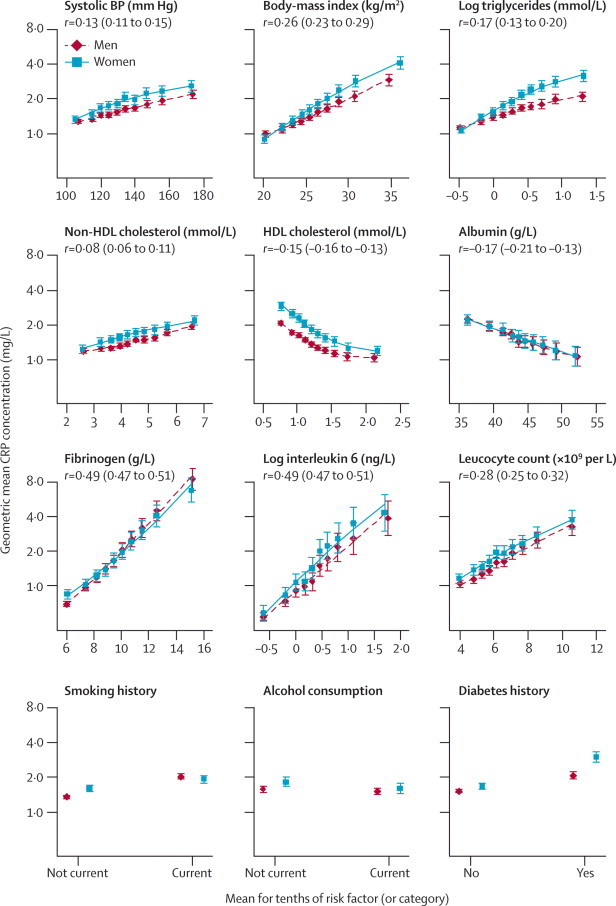
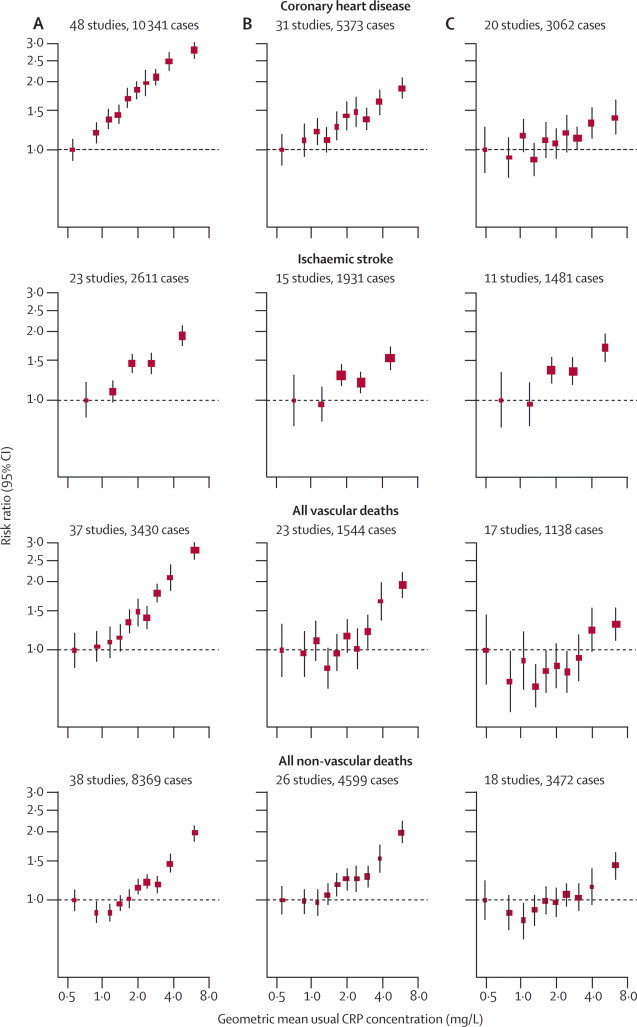
Results: Log(e) CRP concentration was linearly associated with several conventional risk factors and inflammatory markers, and nearly log-linearly with the risk of ischaemic vascular disease and non-vascular mortality. Risk ratios (RRs) for coronary heart disease per 1-SD higher log(e) CRP concentration (three-fold higher) were 1.63 (95% CI 1.51-1.76) when initially adjusted for age and sex only, and 1.37 (1.27-1.48) when adjusted further for conventional risk factors; 1.44 (1.32-1.57) and 1.27 (1.15-1.40) for ischaemic stroke; 1.71 (1.53-1.91) and 1.55 (1.37-1.76) for vascular mortality; and 1.55 (1.41-1.69) and 1.54 (1.40-1.68) for non-vascular mortality. RRs were largely unchanged after exclusion of smokers or initial follow-up. After further adjustment for fibrinogen, the corresponding RRs were 1.23 (1.07-1.42) for coronary heart disease; 1.32 (1.18-1.49) for ischaemic stroke; 1.34 (1.18-1.52) for vascular mortality; and 1.34 (1.20-1.50) for non-vascular mortality.
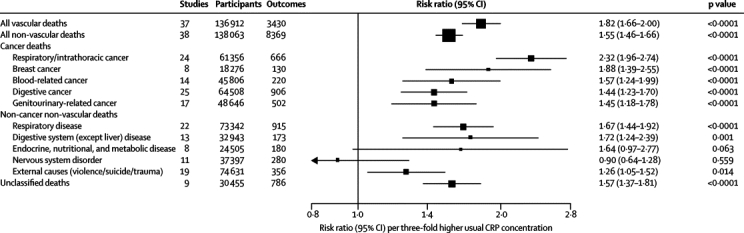
Interpretation: CRP concentration has continuous associations with the risk of coronary heart disease, ischaemic stroke, vascular mortality, and death from several cancers and lung disease that are each of broadly similar size. The relevance of CRP to such a range of disorders is unclear. Associations with ischaemic vascular disease depend considerably on conventional risk factors and other markers of inflammation.
Funding: British Heart Foundation, UK Medical Research Council, BUPA Foundation, and GlaxoSmithKline.
Copyright 2010 Elsevier Ltd. All rights reserved.
Figures
Comment in
-
C-reactive protein and cardiovascular risk: more fuel to the fire.Lancet. 2010 Jan 9;375(9709):95-6. doi: 10.1016/S0140-6736(09)62098-5. Epub 2009 Dec 22. Lancet. 2010. PMID: 20031200 No abstract available.
-
C-reactive protein measurement and cardiovascular disease.Lancet. 2010 Mar 27;375(9720):1078. doi: 10.1016/S0140-6736(10)60470-9. Lancet. 2010. PMID: 20346805 No abstract available.
References
-
- Gabay C, Kushner I. Acute-phase proteins and other systemic responses to inflammation. N Engl J Med. 1999;340:448–454. - PubMed
-
- Emberson JR, Whincup PH, Morris RW, Walker M, Lowe GD, Rumley A. Extent of regression dilution for established and novel coronary risk factors: results from the British Regional Heart Study. Eur J Cardiovasc Prev Rehabil. 2004;11:125–134. - PubMed
-
- Pearson TA, Mensah GA, Alexander RW. Markers of inflammation and cardiovascular disease: application to clinical and public health practice: a statement for healthcare professionals from the Centers for Disease Control and Prevention and the American Heart Association. Circulation. 2003;107:499–511. - PubMed
-
- Kuller LH, Tracy RP, Shaten J, Meilahn EN. Relation of C-reactive protein and coronary heart disease in the MRFIT nested case-control study. Multiple Risk Factor Intervention Trial. Am J Epidemiol. 1996;144:537–547. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
