

Does reducing physician uncertainty improve hypertension control?: rationale and methods
- PMID: 20031846
- PMCID: PMC2780342
- DOI: 10.1161/CIRCOUTCOMES.109.849984
Does reducing physician uncertainty improve hypertension control?: rationale and methods
Abstract
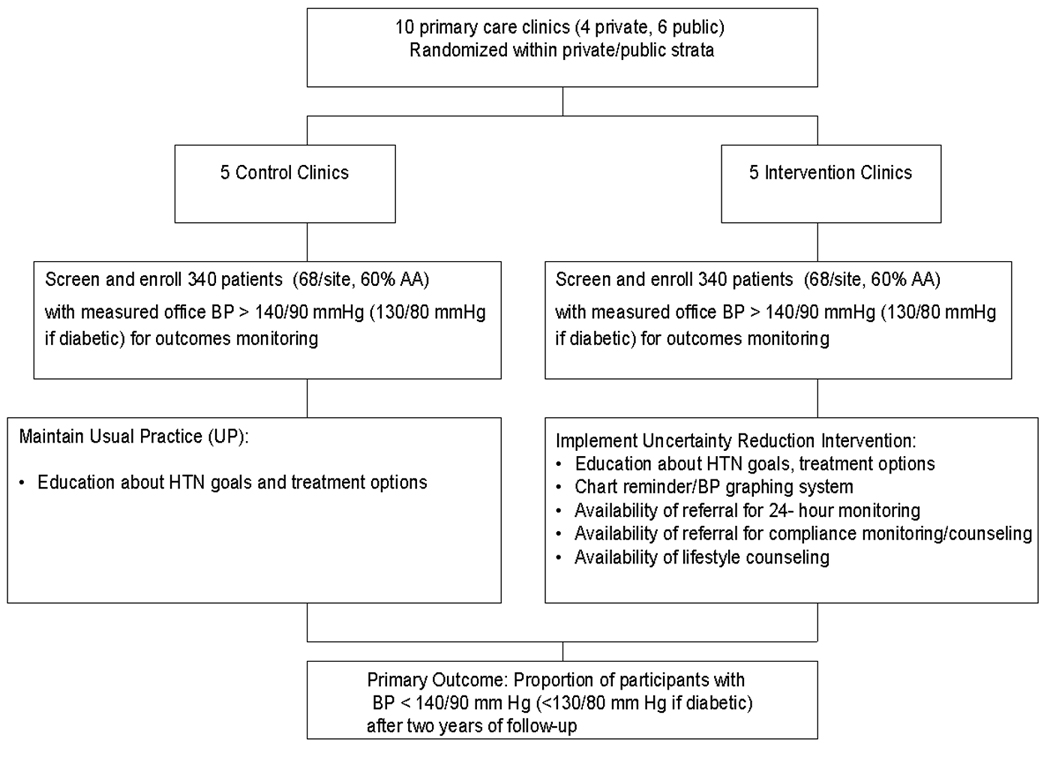
Hypertension affects nearly one third of the US population overall, and the prevalence rises sharply with age. In spite of public educational campaigns and professional education programs to encourage blood pressure measurement and control of both systolic and diastolic control to <140/90 mm Hg (or 130/80 mm Hg if diabetic), 43% of treated hypertensives do not achieve the recommended Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure target. Among blacks, 48% are uncontrolled on treatment. The majority of persons classified as poorly controlled hypertensives have mild systolic blood pressure elevation (in the range of 140 to 160 mm Hg). We hypothesized that physician uncertainty regarding the patient's usual blood pressure, as well as uncertainty regarding the extent of medication nonadherence, represent an important barrier to further reductions in the proportion of uncontrolled hypertensives in the United States. Using cluster randomization, 10 primary care clinics (6 from a public health care system and 4 from a private clinic system) were randomized to either the uncertainty reduction intervention condition or to usual care. An average of 68 patients per clinic were recruited to serve as units of observation. Physicians in the 5 intervention clinics were provided with a specially designed study form that included a graph of recent blood pressure measurements in their study patients, a check box to indicate their assessment of the adequacy of the patient's blood pressure control, and a menu of services they could order to aid in patient management. These menu options included 24-hour ambulatory blood pressure monitoring; electronic bottle cap assessment of medication adherence, followed by medication adherence counseling in patients found to be nonadherent; and lifestyle assessment and counseling followed by 24-hour ambulatory blood pressure monitoring. Physicians in the 5 usual practice clinics did not have access to these services but were informed of which patients had been enrolled in the study. Substudies carried out to further characterize the study population and interpret intervention results included ambulatory blood pressure monitoring and electronic bottle cap monitoring in a random subsample of patients at baseline, and audio recording of patient-physician encounters after intervention implementation. The primary study end point was defined as the proportion of patients with controlled blood pressure (<140/90 mm Hg or <130/80 mm Hg if diabetic). Secondary end points include actual measured clinic systolic and diastolic blood pressure, patient physician communication patterns, physician prescribing patient self-reported lifestyle and medication adherence, physician knowledge, attitude and beliefs regarding the utility of intervention tools to achieve blood pressure control, and the cost-effectiveness of the intervention. Six-hundred eighty patients have been randomized, and 675 remain in active follow-up after 1.5 years. Patient closeout will be complete in March 2009. Analyses of the baseline data are in progress. Office-based blood pressure measurement error and bias, as well as physician and patient beliefs about the need for treatment intensification, may be important factors that limit further progress in blood pressure control. This trial will provide data on the extent to which available technologies not widely used in primary care will change physician prescribing behavior and patient adherence to prescribed treatment.
Similar articles
-
Effect of a physician uncertainty reduction intervention on blood pressure in uncontrolled hypertensives--a cluster randomized trial.J Gen Intern Med. 2012 Apr;27(4):413-9. doi: 10.1007/s11606-011-1888-1. Epub 2011 Oct 27. J Gen Intern Med. 2012. PMID: 22033742 Free PMC article. Clinical Trial.
-
Hypertension Improvement Project (HIP): study protocol and implementation challenges.Trials. 2009 Feb 26;10:13. doi: 10.1186/1745-6215-10-13. Trials. 2009. PMID: 19245692 Free PMC article. Clinical Trial.
-
Folic acid supplementation and malaria susceptibility and severity among people taking antifolate antimalarial drugs in endemic areas.Cochrane Database Syst Rev. 2022 Feb 1;2(2022):CD014217. doi: 10.1002/14651858.CD014217. Cochrane Database Syst Rev. 2022. PMID: 36321557 Free PMC article.
-
Evidence Brief: The Quality of Care Provided by Advanced Practice Nurses [Internet].Washington (DC): Department of Veterans Affairs (US); 2014 Sep. Washington (DC): Department of Veterans Affairs (US); 2014 Sep. PMID: 27606392 Free Books & Documents. Review.
-
An Electronic Adherence Measurement Intervention to Reduce Clinical Inertia in the Treatment of Uncontrolled Hypertension: The MATCH Cluster Randomized Clinical Trial.J Gen Intern Med. 2016 Nov;31(11):1294-1300. doi: 10.1007/s11606-016-3757-4. Epub 2016 Jun 2. J Gen Intern Med. 2016. PMID: 27255750 Free PMC article. Clinical Trial.
Cited by
-
Effect of a physician uncertainty reduction intervention on blood pressure in uncontrolled hypertensives--a cluster randomized trial.J Gen Intern Med. 2012 Apr;27(4):413-9. doi: 10.1007/s11606-011-1888-1. Epub 2011 Oct 27. J Gen Intern Med. 2012. PMID: 22033742 Free PMC article. Clinical Trial.
-
Characteristics, drug combinations and dosages of primary care patients with uncontrolled ambulatory blood pressure and high medication adherence.J Am Soc Hypertens. 2013 Nov-Dec;7(6):471-6. doi: 10.1016/j.jash.2013.06.004. Epub 2013 Jul 23. J Am Soc Hypertens. 2013. PMID: 23890931 Free PMC article. Clinical Trial.
-
The importance of how research participants think they are perceived: results from an electronic monitoring study of antiretroviral therapy in Uganda.AIDS Care. 2019 Jun;31(6):761-766. doi: 10.1080/09540121.2018.1556381. Epub 2018 Dec 9. AIDS Care. 2019. PMID: 30606037 Free PMC article.
-
Toward Standardized Monitoring of Patients With Chronic Diseases in Primary Care Using Electronic Medical Records: Systematic Review.JMIR Med Inform. 2019 May 24;7(2):e10879. doi: 10.2196/10879. JMIR Med Inform. 2019. PMID: 31127717 Free PMC article. Review.
-
Patterns of nonadherence to antihypertensive therapy in primary care.J Clin Hypertens (Greenwich). 2013 Feb;15(2):107-11. doi: 10.1111/jch.12030. Epub 2012 Oct 26. J Clin Hypertens (Greenwich). 2013. PMID: 23339728 Free PMC article.
References
-
- Burt VL, Cutler JA, Higgins M, Horan MJ, Labarthe D, Whelton P, Brown C, Roccella EJ. Trends in the prevalence, awareness, treatment, and control of hypertension in the adult US population. Data from the health examination surveys, 1960 to 1991. Hypertension. 1995;26:60–69. - PubMed
-
- Hajjar I, Kotchen TA. Trends in prevalence, awareness, treatment, and control of hypertension in the United States, 1988–2000. JAMA. 2003;290:199–206. - PubMed
-
- Cutler JA, Sorlie P, Wolz M, Thom T, Fields L, Roccella E. Trends in Hypertension Prevalence, Awareness, Treatment, and Control Rates in United States Adults Between 1988 1994 and 1999 2004. Hypertension. 2008;52:818–827. - PubMed
-
- Berlowitz DR, Ash AS, Hickey EC, Friedman RH, Glickman M, Kader B, Moskowitz MA. Inadequate management of blood pressure in a hypertensive population. N Engl J Med. 1998;339:1957–1963. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
