

Should patient characteristics influence target anticoagulation intensity for stroke prevention in nonvalvular atrial fibrillation?: the ATRIA study
- PMID: 20031854
- PMCID: PMC2801892
- DOI: 10.1161/CIRCOUTCOMES.108.830232
Should patient characteristics influence target anticoagulation intensity for stroke prevention in nonvalvular atrial fibrillation?: the ATRIA study
Abstract
Background: Randomized trials and observational studies support using an international normalized ratio (INR) target of 2.0 to 3.0 for preventing ischemic stroke in atrial fibrillation. We assessed whether the INR target should be adjusted based on selected patient characteristics.
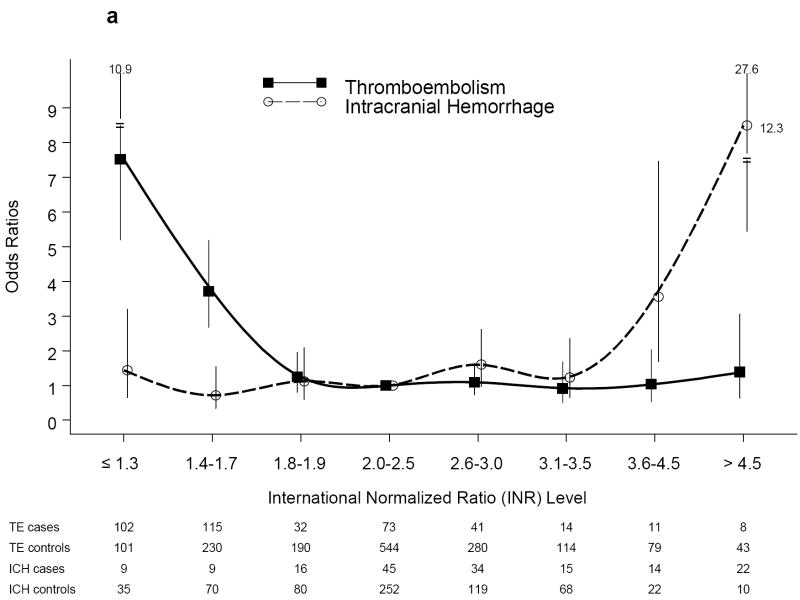
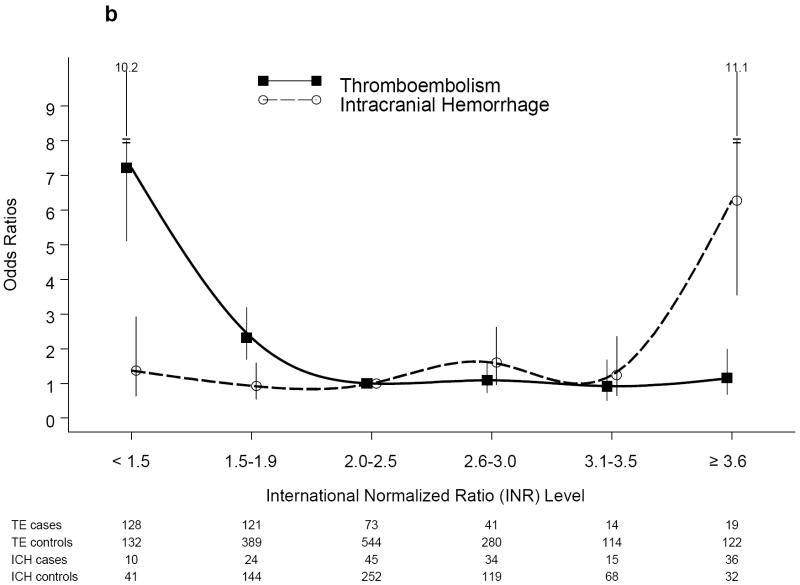
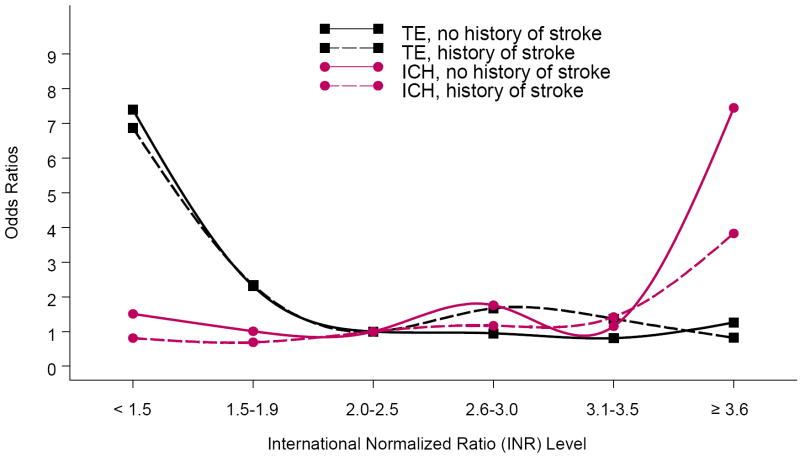
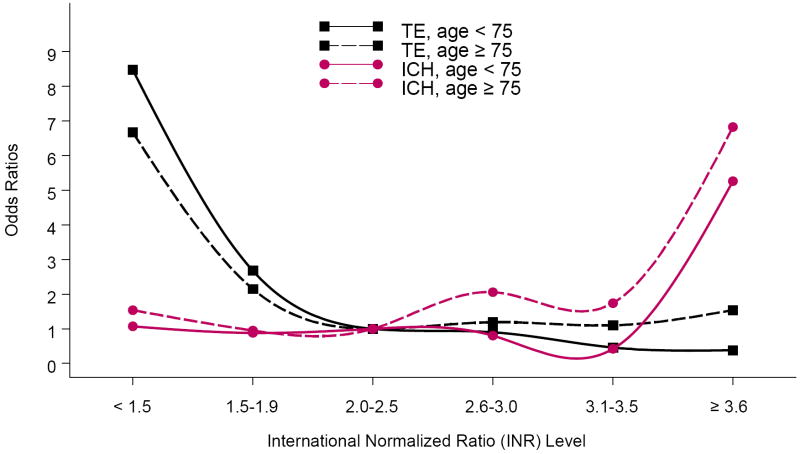
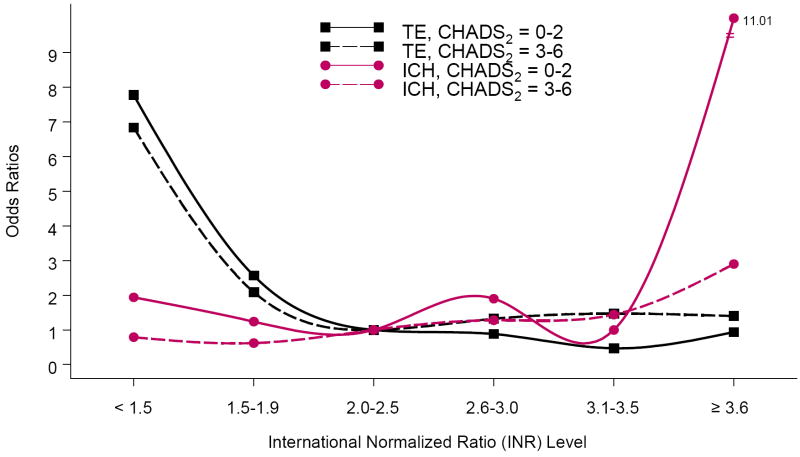
Methods and results: We conducted a case-control study nested within the ATRIA cohort's 9217 atrial fibrillation patients taking warfarin to define the relationship between INR level and the odds of thromboembolism (TE; mainly stroke) and of intracranial hemorrhage (ICH) relative to INR 2.0 to 2.5. We identified 396 TE cases and 164 ICH cases during follow-up. Each case was compared with 4 randomly selected controls matched on calendar date and stroke risk factors using matched univariable analyses and conditional logistic regression. We explored modification of the INR-outcome relationships by the following stroke risk factors: prior stroke, age, and CHADS(2) risk score. Overall, the odds of TE were low and stable above INR 1.8. Compared with INR 2.0 to 2.5, the relative odds of TE increased strikingly at INR <1.8 (eg, odds ratio, 3.72; 95% CI, 2.67 to 5.19, at INR 1.4 to 1.7). The odds of ICH increased markedly at INR values >3.5 (eg, odds ratio, 3.56; 95% CI: 1.70 to 7.46, at INR 3.6 to 4.5). The relative odds of ICH were consistently low at INR <3.6. There was no evidence of lower ICH risk at INR levels <2.0. These patterns of risk did not differ substantially by history of stroke, age, or CHADS(2) risk score.
Conclusions: Our results confirm that the current standard of INR 2.0 to 3.0 for atrial fibrillation falls in the optimal INR range. Our findings do not support adjustment of INR targets according to previously defined stroke risk factors.
Figures
References
-
- Wolf PA, Abbott RD, Kannel WB. Atrial fibrillation: a major contributor to stroke in the elderly: the Framingham Heart Study. Archives of Internal Medicine. 1987;147:1561–1564. - PubMed
-
- Go AS, Hylek EM, Phillips JA, Chang Y, Henault LE, Selby JV, Singer DE. Prevalence of diagnosed atrial fibrillation in adults: National implications for rhythm management and stroke prevention: the AnTicoagulation and Risk Factors in Atrial Fibrillation (ATRIA) Study. JAMA. 2001;285:2370–2375. - PubMed
-
- Go AS, Hylek EM, Chang Y, Phillips KA, Henault LE, Capra AM, Jensvold NG, Selby JV, Singer DE. Anticoagulation therapy for stroke prevention in atrial fibrillation: how well do randomized trials translate into clinical practice? JAMA. 2003 Nov 26;290:2685–2692. - PubMed
-
- Risk factors for stroke and efficacy of antithrombotic therapy in atrial fibrillation. Analysis of pooled data from five randomized controlled trials. Arch Intern Med. 1994 Jul 11;154:1449–1457. - PubMed
-
- Fang MC, Chang Y, Hylek EM, Rosand J, Greenberg SM, Go AS, Singer DE. Advanced age, anticoagulation intensity, and risk for intracranial hemorrhage among patients taking warfarin for atrial fibrillation. Ann Intern Med. 2004 Nov 16;141:745–752. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
