

The association of cognitive and somatic depressive symptoms with depression recognition and outcomes after myocardial infarction
- PMID: 20031858
- PMCID: PMC2779543
- DOI: 10.1161/CIRCOUTCOMES.109.868588
The association of cognitive and somatic depressive symptoms with depression recognition and outcomes after myocardial infarction
Abstract
Background: Among patients with acute myocardial infarction (AMI), depression is both common and underrecognized. The association of different manifestations of depression, somatic and cognitive, with depression recognition and long-term prognosis is poorly understood.
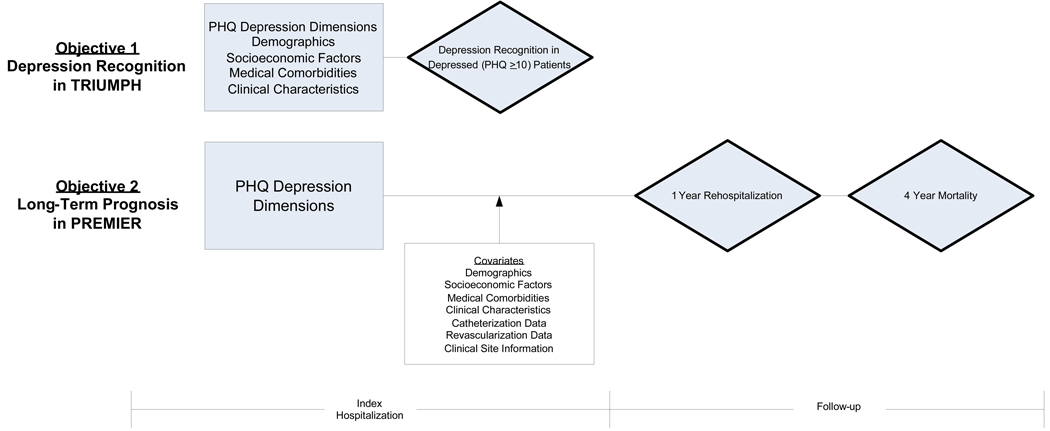
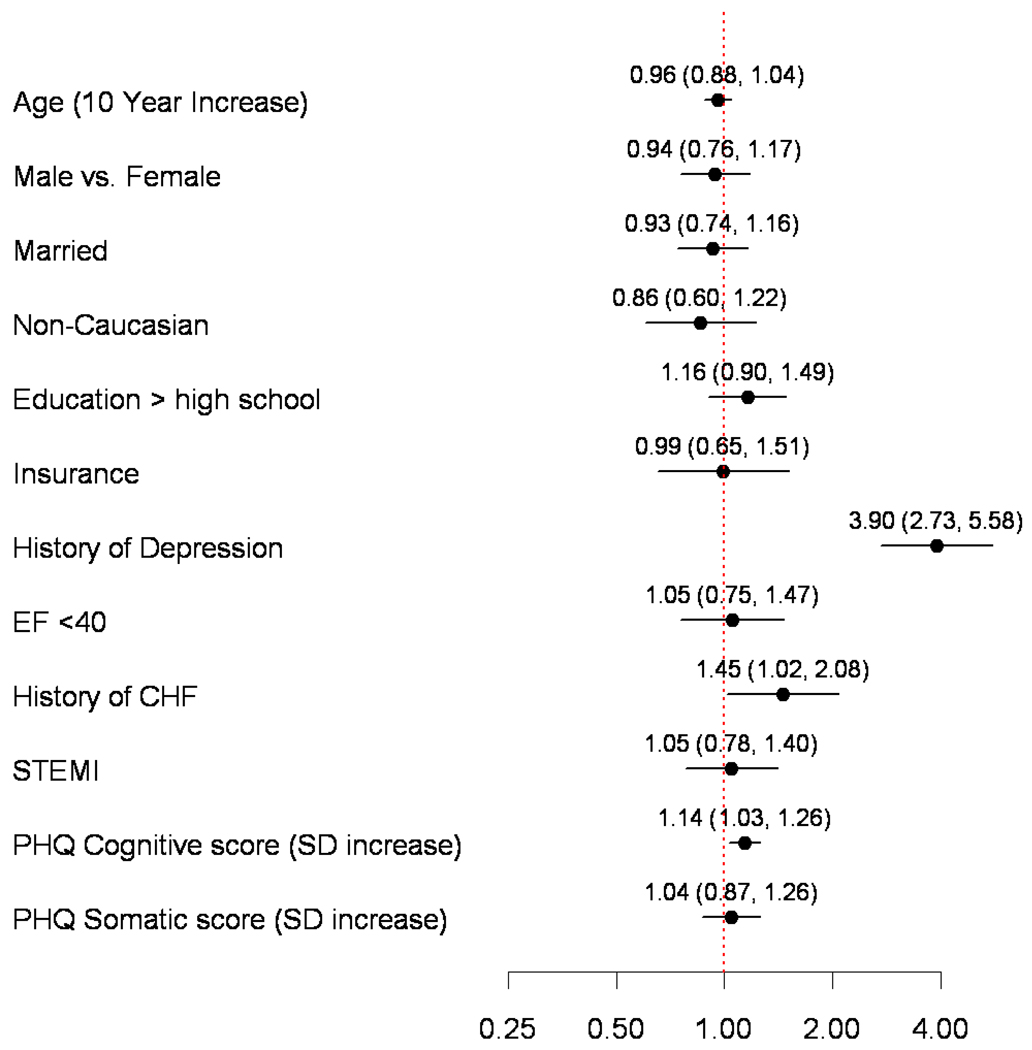
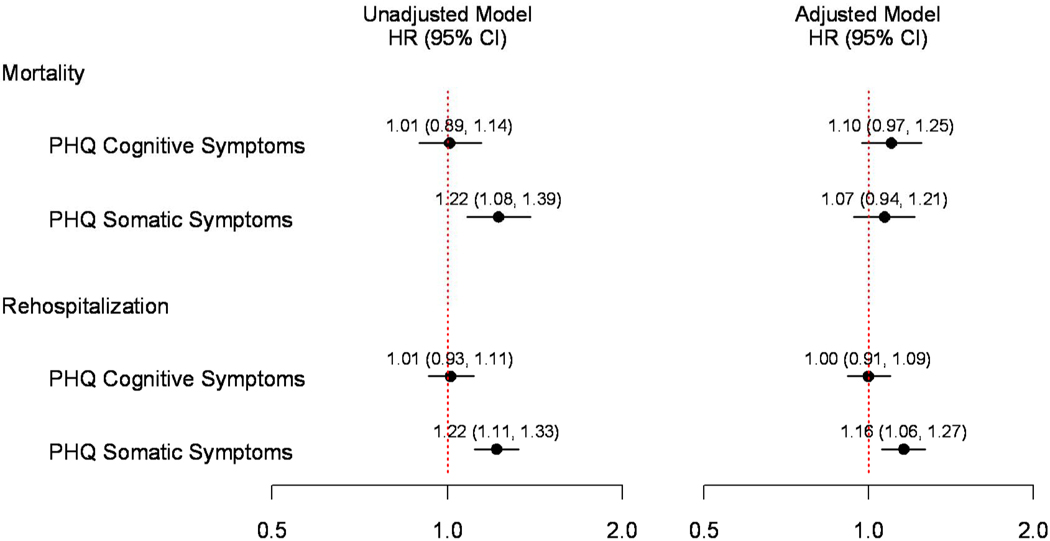
Methods and results: Depression was confirmed in 481 AMI patients enrolled from 21 sites during their index hospitalization with a Patient Health Questionnaire (PHQ-9) score > or =10. Within the PHQ-9, separate somatic and cognitive symptom scores were derived, and the independent association between these domains and the clinical recognition of depression, as documented in the medical records, was evaluated. In a separate multisite AMI registry of 2347 patients, the association between somatic and cognitive depressive symptoms and 4-year all-cause mortality and 1-year all-cause rehospitalization was evaluated. Depression was clinically recognized in 29% (n=140) of patients. Cognitive depressive symptoms (relative risk per SD increase, 1.14; 95% CI, 1.03 to 1.26; P=0.01) were independently associated with depression recognition, whereas the association for somatic symptoms and recognition (relative risk, 1.04; 95% CI, 0.87 to 1.26; P=0.66) was not significant. However, unadjusted Cox regression analyses found that only somatic depressive symptoms were associated with 4-year mortality (hazard ratio [HR] per SD increase, 1.22; 95% CI, 1.08 to 1.39) or 1-year rehospitalization (HR, 1.22; 95% CI, 1.11 to 1.33), whereas cognitive manifestations were not (HR for mortality, 1.01; 95% CI, 0.89 to 1.14; HR for rehospitalization, 1.01; 95% CI, 0.93 to 1.11). After multivariable adjustment, the association between somatic symptoms and rehospitalization persisted (HR, 1.16; 95% CI, 1.06 to 1.27; P=0.01) but was attenuated for mortality (HR, 1.07; 95% CI, 0.94 to 1.21; P=0.30).
Conclusions: Depression after AMI was recognized in fewer than 1 in 3 patients. Although cognitive symptoms were associated with recognition of depression, somatic symptoms were associated with long-term outcomes. Comprehensive screening and treatment of both somatic and cognitive symptoms may be necessary to optimize depression recognition and treatment in AMI patients.
Conflict of interest statement
None.
Figures
References
-
- Frasure-Smith N, Lesperance F. Recent evidence linking coronary heart disease and depression. Can J Psychiatry. 2006;51:730–737. - PubMed
-
- Barth J, Schumacher M, Herrmann-Lingen C. Depression as a risk factor for mortality in patients with coronary heart disease: a meta-analysis. Psychosom Med. 2004;66:802–813. - PubMed
-
- Carney RM, Blumenthal JA, Catellier D, Freedland KE, Berkman LF, Watkins LL, Czajkowski SM, Hayeno J, Jaffe AS. Depression as a risk factor for mortality after acute myocardial infarction. Am J Cardiol. 2003;92:1277–1281. - PubMed
-
- Parashar S, Rumsfeld JS, Spertus JA, Reid KJ, Wenger NK, Krumholz HM, Amin A, Weintraub WS, Lichtman J, Dawood N, Vaccarino V. Time course of depression and outcome of myocardial infarction. Arch Intern Med. 2006;166:2035–2043. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
