

Incidence and risk factors of HIV-related non-Hodgkin's lymphoma in the era of combination antiretroviral therapy: a European multicohort study
- PMID: 20032536
- PMCID: PMC2821596
- DOI: 10.3851/IMP1462
Incidence and risk factors of HIV-related non-Hodgkin's lymphoma in the era of combination antiretroviral therapy: a European multicohort study
Abstract
Background: Incidence and risk factors of HIV-associated non-Hodgkin's lymphoma (NHL) are not well defined in the era of combination antiretroviral therapy (cART).
Methods: A total of 56,305 adult HIV type-1 (HIV-1)-infected patients who started cART in 1 of 22 prospective studies in Europe were included. Weibull random effects models were used to estimate hazard ratios (HRs) for developing systemic NHL and included CD4(+) T-cell counts and viral load as time-updated variables.
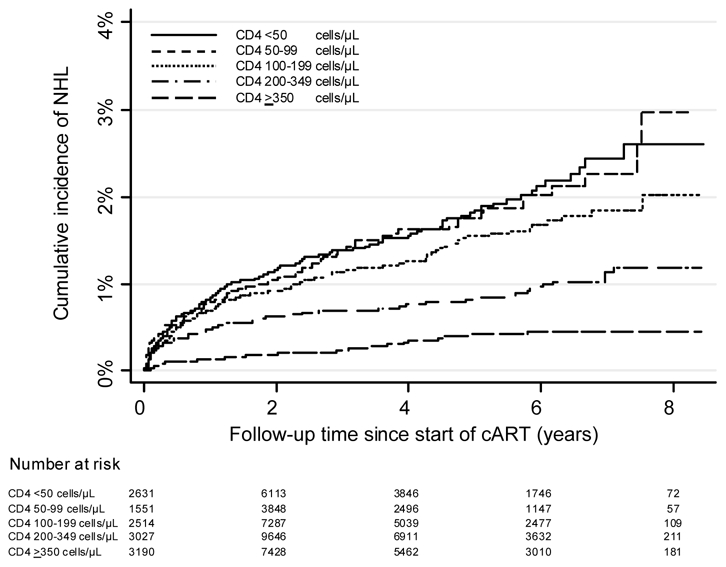
Results: During the 212,042 person-years of follow-up, 521 patients were diagnosed with systemic NHL and 62 with primary brain lymphoma (PBL). The incidence rate of systemic NHL was 463 per 100,000 person-years not on cART and 205 per 100,000 person-years in treated patients for a rate ratio of 0.44 (95% confidence interval [CI] 0.37-0.53). The corresponding incidence rates of PBL were 57 and 24 per 100,000 person-years (rate ratio 0.43, 95% CI 0.25-0.73). Suppression of HIV-1 replication on cART (HR 0.60, 95% CI 0.44-0.81, comparing < or =500 with 10,000-99,999 copies/ml) and increases in CD4(+) T-cell counts (HR 0.30, 0.22-0.42, comparing > or =350 with 100-199 cells/microl) were protective; a history of Kaposi's sarcoma (HR 1.70, 1.08-2.68, compared to no history of AIDS), transmission through sex between men (HR 1.57, 1.19-2.08, compared with heterosexual transmission) and older age (HR 3.71, 2.37-5.80, comparing > or =50 with 16-29 years) were risk factors for systemic NHL.
Conclusions: The incidence rates of both systemic NHL and PBL were substantially reduced in patients on cART. Timely initiation of therapy is key to the prevention of NHL in the era of cART.
Figures


References
-
- Dal Maso L, Franceschi S. Epidemiology of non-Hodgkin lymphomas and other haemolymphopoietic neoplasms in people with AIDS. Lancet Oncol. 2003;4:110–119. - PubMed
-
- Frisch M, Biggar RJ, Engels EA, Goedert JJ. Association of cancer with AIDS-related immunosuppression in adults. JAMA. 2001;285:1736–1745. - PubMed
-
- Cote TR, Biggar RJ, Rosenberg PS, et al. Non-Hodgkin’s lymphoma among people with AIDS: incidence, presentation and public health burden. AIDS/Cancer Study Group. Int J Cancer. 1997;73:645–650. - PubMed
-
- Ledergerber B, Egger M, Erard V, et al. AIDS-related opportunistic illnesses occurring after initiation of potent antiretroviral therapy: the Swiss HIV Cohort Study. JAMA. 1999;282:2220–2226. - PubMed
-
- Engels EA, Biggar RJ, Hall HI, et al. Cancer risk in people infected with human immunodeficiency virus in the United States. Int J Cancer. 2008;123:187–194. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
