

HIV replication capacity is an independent predictor of disease progression in persons with untreated chronic HIV infection
- PMID: 20032783
- PMCID: PMC2837106
- DOI: 10.1097/QAI.0b013e3181cae480
HIV replication capacity is an independent predictor of disease progression in persons with untreated chronic HIV infection
Abstract
Objective: To assess the effect of pol replication capacity (RC) on the hazard ratio of progression to a composite endpoint of time to progression to <350 CD4+ cells per microliter, initiation of therapy, or death.
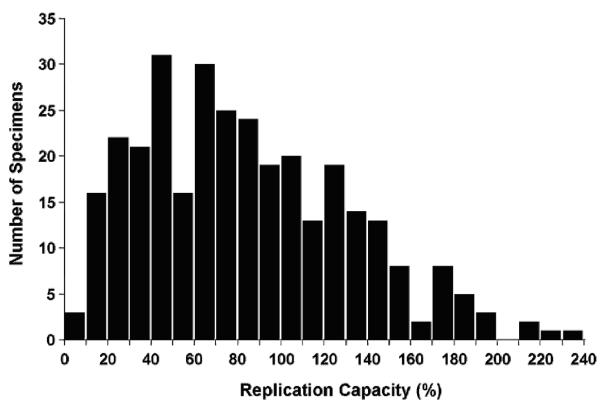
Methods: pol RC assays were performed after study closure in baseline samples obtained from 316 enrollees in a prospectively monitored cohort of treatment-naive adults with >or=450 CD4+ cells per microliter and >or=1000 HIV-1 RNA copies per milliliter.
Results: The median RC was 79%. Patients with a lower RC had a lower median viral load (4.0 vs 4.2 Log HIV-1 RNA copies/mL, P = 0.026) and a lower rate of protease inhibitor resistance 2% vs 8%, P = 0.03). Otherwise, baseline demographic and laboratory characteristics were similar. The hazard ratio of progression to the composite endpoint was 0.73 (P = 0.041) for persons with lower RC, 2.07 per 1.0 log10 higher viral load (P < 0.001), and 0.86 per 50 cells per microliter higher CD4+ cell count (P < 0.001). The effect of lower RC was also significant in a separate analysis of time to initiation of therapy (P = 0.04).
Conclusions: These results show that untreated patients with lower vs higher RC had a slower rate of progression as assessed by a composite outcome of time to CD4+ count <or=350 cells per microliter, treatment initiation, or death.
Keywords: HIV infections; disease progression; natural history; replication.
Figures

Similar articles
-
Relationship between HIV coreceptor tropism and disease progression in persons with untreated chronic HIV infection.J Acquir Immune Defic Syndr. 2009 Mar 1;50(3):259-66. doi: 10.1097/QAI.0b013e3181989a8b. J Acquir Immune Defic Syndr. 2009. PMID: 19194318 Free PMC article.
-
HIV type 1 polymerase gene polymorphisms are associated with phenotypic differences in replication capacity and disease progression.J Infect Dis. 2014 Jan 1;209(1):66-73. doi: 10.1093/infdis/jit425. Epub 2013 Aug 6. J Infect Dis. 2014. PMID: 23922373 Free PMC article.
-
Higher CD4+ T cell counts associated with low viral pol replication capacity among treatment-naive adults in early HIV-1 infection.J Infect Dis. 2004 Jul 15;190(2):251-6. doi: 10.1086/422036. Epub 2004 Jun 18. J Infect Dis. 2004. PMID: 15216458
-
Pol-Driven Replicative Capacity Impacts Disease Progression in HIV-1 Subtype C Infection.J Virol. 2018 Sep 12;92(19):e00811-18. doi: 10.1128/JVI.00811-18. Print 2018 Oct 1. J Virol. 2018. PMID: 29997209 Free PMC article.
-
Determinants of the natural history of human immunodeficiency virus type 1 infection.J Infect Dis. 1999 Mar;179 Suppl 2:S384-6. doi: 10.1086/513839. J Infect Dis. 1999. PMID: 10081512 Review.
Cited by
-
Treatment-associated polymorphisms in protease are significantly associated with higher viral load and lower CD4 count in newly diagnosed drug-naive HIV-1 infected patients.Retrovirology. 2012 Oct 3;9:81. doi: 10.1186/1742-4690-9-81. Retrovirology. 2012. PMID: 23031662 Free PMC article.
-
Lack of a significant impact of Gag-Protease-mediated HIV-1 replication capacity on clinical parameters in treatment-naive Japanese individuals.Retrovirology. 2015 Nov 19;12:98. doi: 10.1186/s12977-015-0223-z. Retrovirology. 2015. PMID: 26585907 Free PMC article.
-
Factors Associated With the Control of Viral Replication and Virologic Breakthrough in a Recently Infected HIV-1 Controller.EBioMedicine. 2017 Feb;16:141-149. doi: 10.1016/j.ebiom.2017.01.034. Epub 2017 Jan 26. EBioMedicine. 2017. PMID: 28159573 Free PMC article.
-
Early virologic failure and the development of antiretroviral drug resistance mutations in HIV-infected Ugandan children.J Acquir Immune Defic Syndr. 2011 Jan 1;56(1):44-50. doi: 10.1097/QAI.0b013e3181fbcbf7. J Acquir Immune Defic Syndr. 2011. PMID: 21099693 Free PMC article.
-
A Novel High Throughput, Parallel Infection Assay for Determining the Replication Capacities of 346 Primary HIV-1 Isolates of the Zurich Primary HIV-1 Infection Study in Primary Cells.Viruses. 2021 Mar 4;13(3):404. doi: 10.3390/v13030404. Viruses. 2021. PMID: 33806576 Free PMC article.
References
-
- DHHS Panel on Antiretroviral Guidelines for Adults and Adolescents Guidelines for the Use of Antiretroviral Agents in HIV-infected adults and adolescents. Nov 4, 2008. Available at http://aidsinfo.nih.gov/contentfiles/AdultandAdolescentGL.pdf.
-
- Lyles RH, Munoz A, Yamashita TE, et al. Natural history of human immunodeficiency virus type 1 viremia after seroconversion and proximal to AIDS in a large cohort of homosexual men. Multicenter AIDS Cohort Study. J Infect Dis. 2000;181:872–80. - PubMed
-
- Rodriguez B, Sethi AK, Cheruvu VK, et al. Predictive value of plasma HIV RNA level on rate of CD4 T-cell decline in untreated HIV infection. JAMA. 2006;296:1498–506. - PubMed
-
- Learmont JC, Geczy AF, Mills J, et al. Immunologic and virologic status after 14 to 18 years of infection with an attenuated strain of HIV-1. A report from the Sydney Blood Bank Cohort. N Engl J Med. 1999;340:1715–22. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
