

Phenotypic characteristics and diagnoses of patients referred to an iron overload clinic
- PMID: 20033846
- PMCID: PMC3481540
- DOI: 10.1007/s10620-009-1080-1
Phenotypic characteristics and diagnoses of patients referred to an iron overload clinic
Abstract
Background: There are limited data on the phenotypic differences between patients with hereditary hemochromatosis (HH) and other forms of iron overload.
Aims: To describe and compare patients suspected of having iron overload disease.
Methods: Patients were evaluated at a university iron overload clinic over a 5-year period. Biochemical and clinical profiles of patients with HH and non-HH causes of suspected iron overload were retrospectively compared.
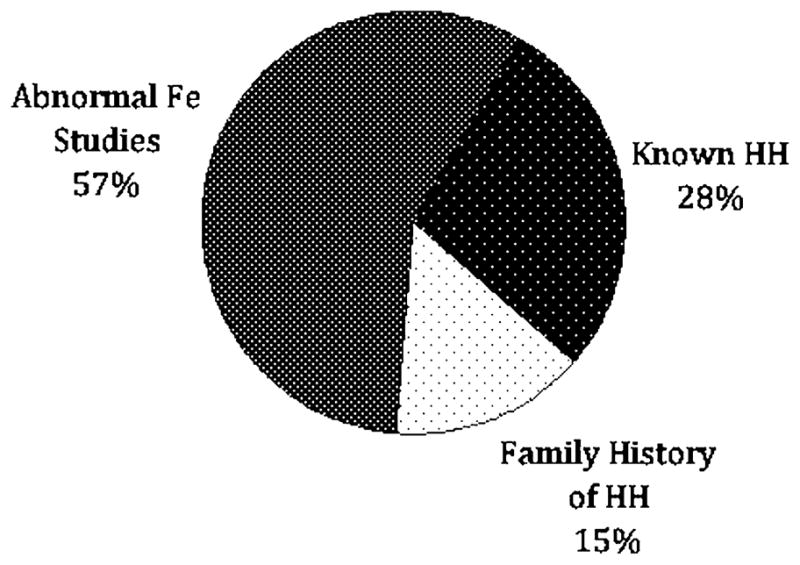
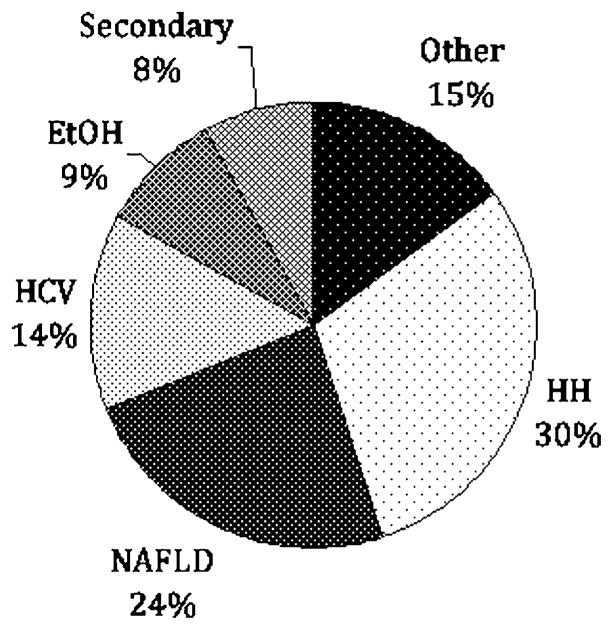
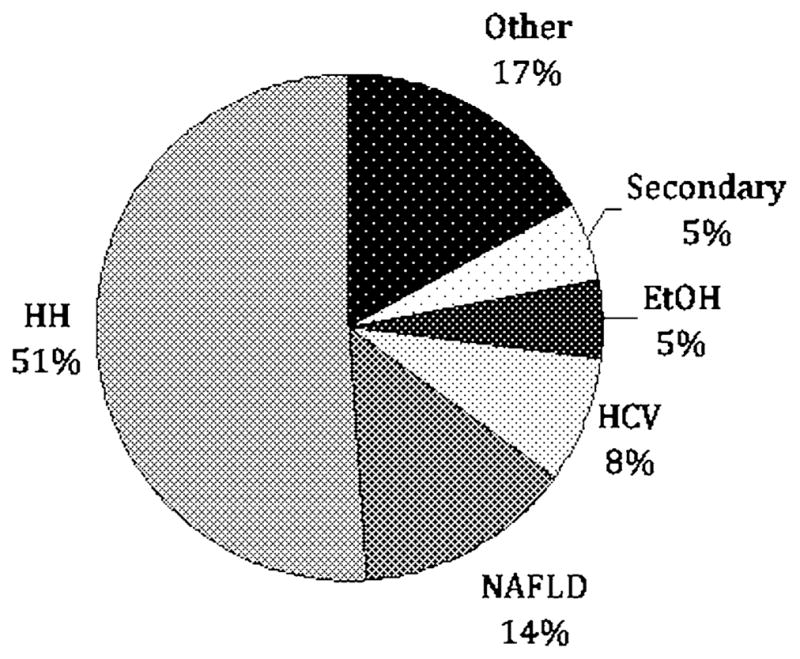
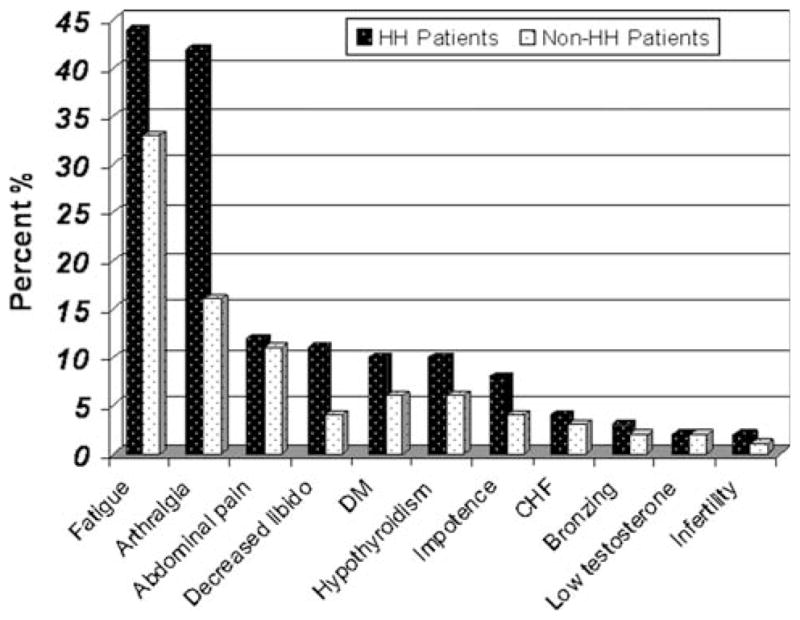
Results: A total of 270 patients were evaluated during the enrollment period, and 137 (51%) were diagnosed with HH. The most common reasons for referral were elevated serum iron markers (155 patients), followed by positive family history (40 patients), and known HH (75 patients). In patients without HH referred for suspected iron overload, the most common diagnoses were nonalcoholic fatty liver disease (NAFLD) (24%), chronic hepatitis C infection (14%), and alcohol related liver disease (9%). Of the patients with HH, 108 were C282Y homozygotes, 20 were compound heterozygotes (C282Y/H63D), and nine had neither mutation. The following clinical characteristics were significantly different (p < 0.05) between patients with HH and all other referred patients: arthralgia (42 vs. 16%) and decreased libido (11 vs. 4%). There was a non-significant trend towards increased fatigue (44 vs. 33%), diabetes (10 vs. 6%), impotence (8 vs. 4%), and hypothyroidism (10 vs. 6%) in the HH group.
Conclusions: (1) A large proportion of patients referred for suspected iron overload have diagnoses other than HH. (2) NAFLD, chronic hepatitis C, and chronic alcohol use were the most common alternative diagnoses. (3) Arthralgia and fatigue are the most common symptoms among patients with HH.
Conflict of interest statement
Figures
References
-
- Gurrin LC, Osborne NJ, Constantine CC, et al. The natural history of serum iron indices for HFE C282Y homozygosity associated with hereditary hemochromatosis. Gastroenterology. 2008;135:1945–1952. - PubMed
-
- Beutler E, Felitti JVJ, Koziol JA, et al. Penetrance of the 845G → A (C282Y) HFE hereditary haemochromatosis mutation in the USA. Lancet. 2002;359:211–218. - PubMed
-
- Allen KJ, Gurrin LC, Constantine CC, et al. Iron-overload-related disease in HFE hereditary hemochromatosis. N Engl J Med. 2008;358:221–230. - PubMed
-
- Yen AW, Fancher TL, Bowlus CL. Revisiting hereditary hemochromatosis: current concepts and progress. Am J Med. 2006;119:391–399. - PubMed
-
- Alexander J, Kowdley KV. HFE-associated hereditary hemochromatosis. Genet Med. 2009;11:307–313. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
