

Role of ADAM and ADAMTS metalloproteinases in airway diseases
- PMID: 20034386
- PMCID: PMC2805617
- DOI: 10.1186/1465-9921-10-127
Role of ADAM and ADAMTS metalloproteinases in airway diseases
Abstract
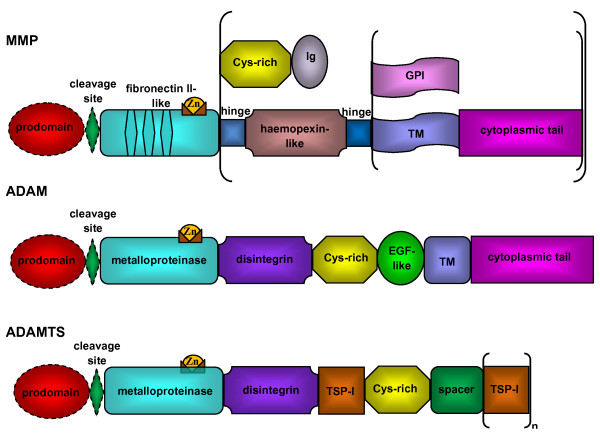
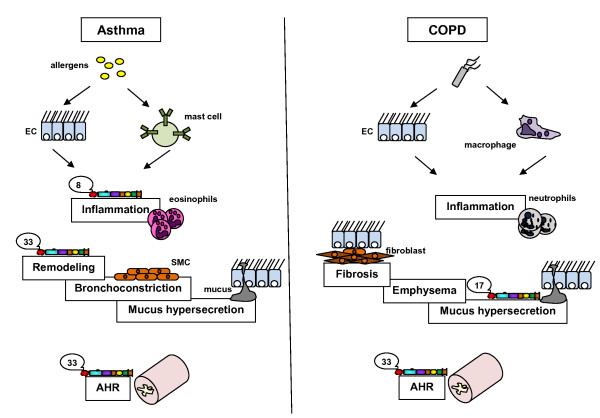
Lungs are exposed to the outside environment and therefore to toxic and infectious agents or allergens. This may lead to permanent activation of innate immune response elements. A Disintegrin And Metalloproteinases (ADAMs) and ADAMs with Thrombospondin motifs (ADAMTS) are proteinases closely related to Matrix Metalloproteinases (MMPs). These multifaceted molecules bear metalloproteinase and disintegrin domains endowing them with features of both proteinases and adhesion molecules. Proteinases of the ADAM family are associated to various physiological and pathological processes and display a wide spectrum of biological effects encompassing cell fusion, cell adhesion, "shedding process", cleavage of various substrates from the extracellular matrix, growth factors or cytokines... This review will focus on the putative roles of ADAM/ADAMTS proteinases in airway diseases such as asthma and COPD.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
