

Lynch syndrome among gynecologic oncology patients meeting Bethesda guidelines for screening
- PMID: 20034658
- PMCID: PMC2822124
- DOI: 10.1016/j.ygyno.2009.11.021
Lynch syndrome among gynecologic oncology patients meeting Bethesda guidelines for screening
Abstract
Objective: Lynch syndrome (LS) is characterized by a high lifetime incidence of colorectal cancer and gynecologic malignancies such as endometrial and ovarian cancer. Identification of LS families is important as it allows for heightened cancer screening which decreases colorectal cancer mortality. The original 1996 Bethesda guidelines included two gynecologic populations that should be further evaluated for LS: those with endometrial cancer before the age of 45 years and those with two LS-related cancers (i.e. synchronous endometrial and ovarian cancer). Our study aims to estimate the prevalence of LS in these two populations.
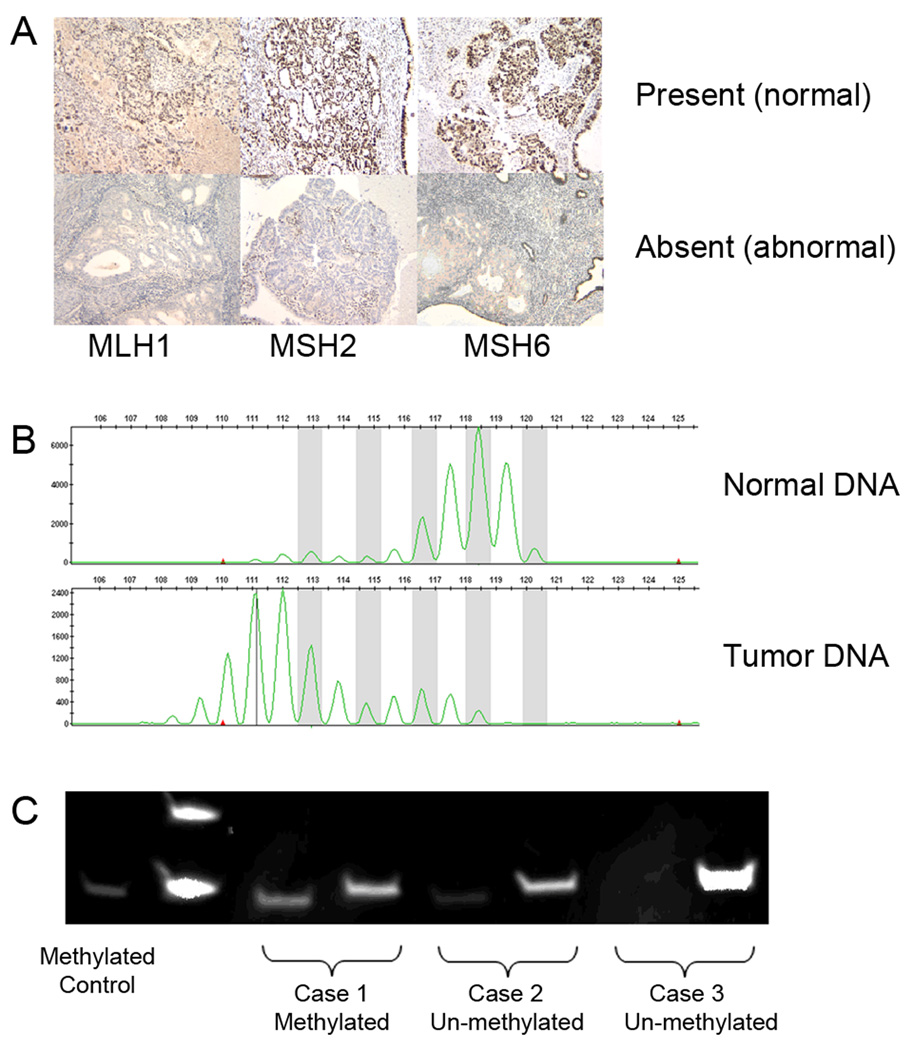
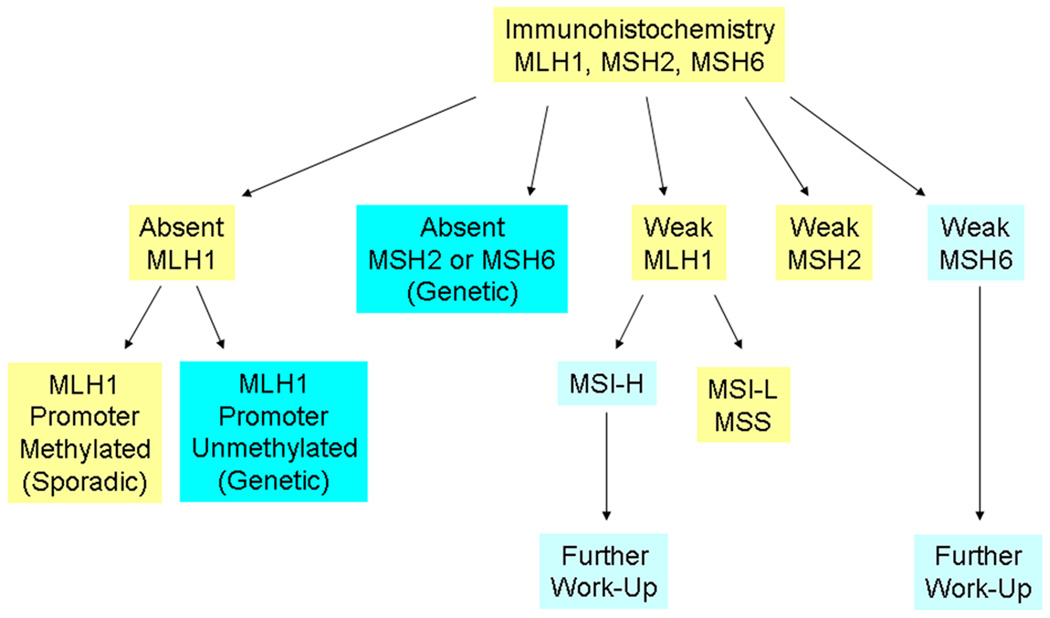
Methods: We utilized a diagnostic algorithm that included immunohistochemistry for mismatch repair protein expression followed by selective evaluation for microsatellite instability and MLH1 gene promoter methylation.
Results: Among 72 eligible patients, 9 (12%) had molecular findings consistent with LS: 6/50 (12%) in the early-onset endometrial cancer group and 3/22 (14%) in the synchronous primary cancer group. In an additional 3 cases, MLH1 silencing was due to promoter methylation: 1/50 (2%) in the early-onset endometrial cancer group and 2/22 (9%) in the synchronous primary cancer group. Of the 9 women with molecular criteria suggesting LS, only three had pedigrees meeting the Amsterdam criteria.
Conclusions: A diagnostic algorithm can identify patients with LS and those who warrant further genetic testing. Our findings reinforce the recommendation that women diagnosed with endometrial cancer before the age of 45 years and women with synchronous endometrial and ovarian cancer be screened for LS, irrespective of family history.
Conflict of interest statement
Conflict of Interest Statement: There are no financial disclosures from any authors.
Figures
Similar articles
-
Combined Microsatellite Instability, MLH1 Methylation Analysis, and Immunohistochemistry for Lynch Syndrome Screening in Endometrial Cancers From GOG210: An NRG Oncology and Gynecologic Oncology Group Study.J Clin Oncol. 2015 Dec 20;33(36):4301-8. doi: 10.1200/JCO.2015.63.9518. Epub 2015 Nov 9. J Clin Oncol. 2015. PMID: 26552419 Free PMC article.
-
Comparison of screening strategies for Lynch syndrome in patients with newly diagnosed endometrial cancer: a prospective cohort study in China.Cancer Commun (Lond). 2019 Jul 15;39(1):42. doi: 10.1186/s40880-019-0388-2. Cancer Commun (Lond). 2019. PMID: 31307542 Free PMC article.
-
Implementation of tumor testing for lynch syndrome in endometrial cancers at a large academic medical center.Gynecol Oncol. 2013 Jul;130(1):121-6. doi: 10.1016/j.ygyno.2013.04.022. Epub 2013 Apr 20. Gynecol Oncol. 2013. PMID: 23612316
-
Lynch syndrome presenting as endometrial cancer.Clin Chem. 2014 Jan;60(1):111-21. doi: 10.1373/clinchem.2013.206888. Epub 2013 Nov 5. Clin Chem. 2014. PMID: 24193118 Review.
-
[Colorectal Carcinoma with Suspected Lynch Syndrome: A Multidisciplinary Algorithm].Zentralbl Chir. 2015 Dec;140(6):591-9. doi: 10.1055/s-0034-1368480. Epub 2014 Nov 5. Zentralbl Chir. 2015. PMID: 25372301 Review. German.
Cited by
-
The Role of Immunohistochemistry Markers in Endometrial Cancer with Mismatch Repair Deficiency: A Systematic Review.Cancers (Basel). 2022 Aug 3;14(15):3783. doi: 10.3390/cancers14153783. Cancers (Basel). 2022. PMID: 35954447 Free PMC article. Review.
-
Identification of Lynch Syndrome in Patients with Endometrial Cancer Based on a Germline Next Generation Sequencing Multigene Panel Test.Cancers (Basel). 2022 Jul 13;14(14):3406. doi: 10.3390/cancers14143406. Cancers (Basel). 2022. PMID: 35884469 Free PMC article.
-
Familial cancer among consecutive uterine cancer patients in Sweden.Hered Cancer Clin Pract. 2014 May 7;12(1):14. doi: 10.1186/1897-4287-12-14. eCollection 2014. Hered Cancer Clin Pract. 2014. PMID: 24851142 Free PMC article.
-
Mismatch repair protein expression in 1049 endometrial carcinomas, associations with body mass index, and other clinicopathologic variables.Gynecol Oncol. 2014 Apr;133(1):43-7. doi: 10.1016/j.ygyno.2014.01.017. Epub 2014 Jan 17. Gynecol Oncol. 2014. PMID: 24444820 Free PMC article.
-
Lynch syndrome screening should be considered for all patients with newly diagnosed endometrial cancer.Am J Surg Pathol. 2014 Nov;38(11):1501-9. doi: 10.1097/PAS.0000000000000321. Am J Surg Pathol. 2014. PMID: 25229768 Free PMC article.
References
-
- Dunlop MG, Farrington SM, Carothers AD, et al. Cancer risk associated with germline DNA mismatch repair gene mutations. Hum Mol Genet. 1997;6(1):105–110. - PubMed
-
- Aarnio M, Sankila R, Pukkala E, et al. Cancer risk in mutation carriers of DNA-mismatch-repair genes. Int J Cancer. 1999;81(2):214–218. - PubMed
-
- Watson P, Lynch HT. Extracolonic cancer in hereditary nonpolyposis colorectal cancer. Cancer. 1993;71(3):677–685. - PubMed
-
- Jarvinen HJ, Aarnio M, Mustonen H, et al. Controlled 15-year trial on screening for colorectal cancer in families with hereditary nonpolyposis colorectal cancer. Gastroenterology. 2000;118(5):829–834. - PubMed
-
- Vasen HF, Mecklin JP, Khan PM, et al. The International Collaborative Group on Hereditary Non-Polyposis Colorectal Cancer (ICG-HNPCC) Dis Colon Rectum. 1991;34(5):424–425. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
