

Single-incision laparoscopic cholecystectomy: initial evaluation of a large series of patients
- PMID: 20035355
- PMCID: PMC2869438
- DOI: 10.1007/s00464-009-0786-7
Single-incision laparoscopic cholecystectomy: initial evaluation of a large series of patients
Abstract
Background: Findings have shown that single-incision laparoscopic cholecystectomy (SILC) is feasible and reproducible. The authors have pioneered a two-trocar SILC technique at the University of Texas Southwestern. Their results for 100 patients are presented.
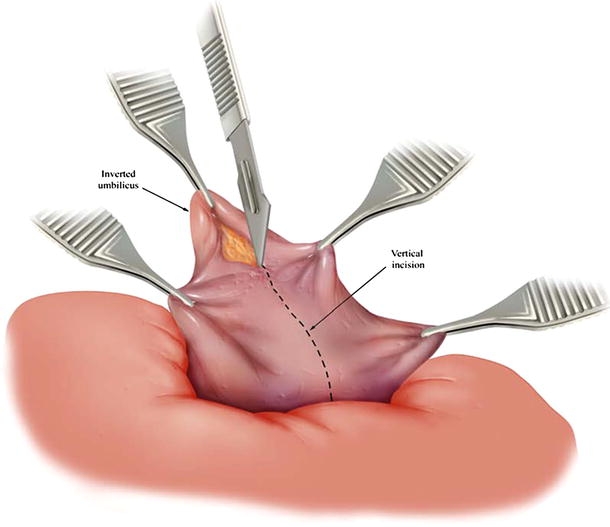
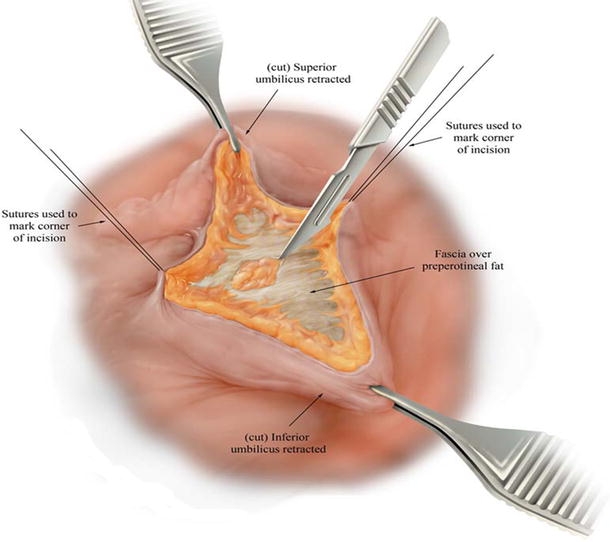
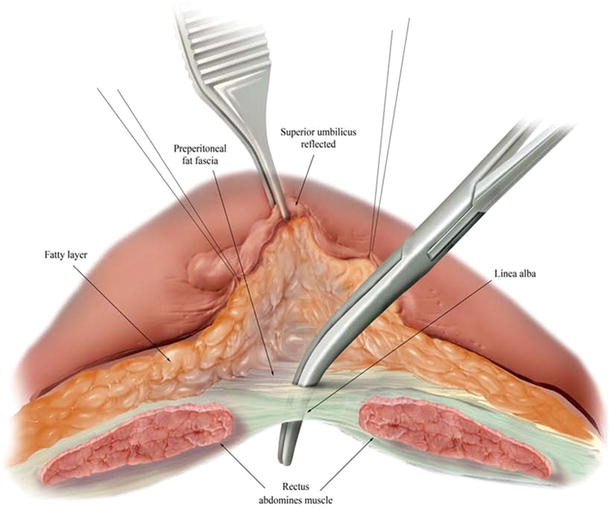
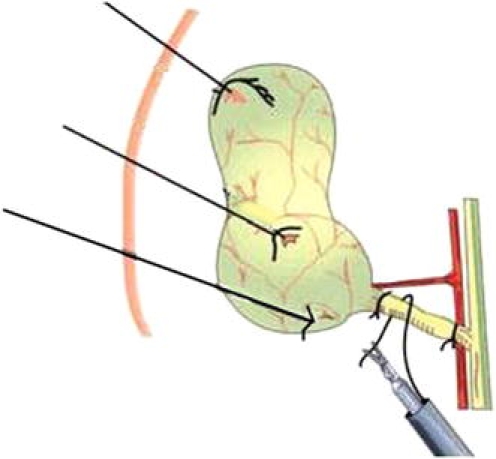
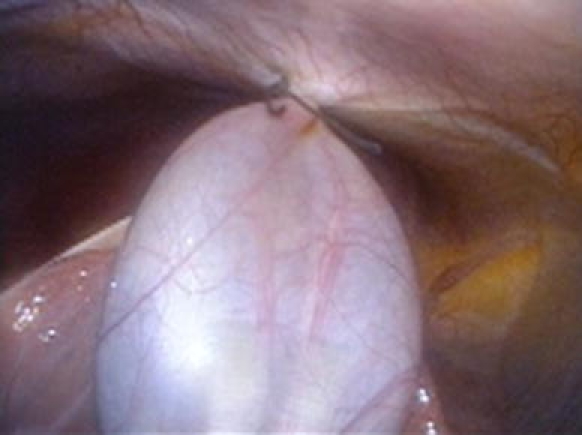
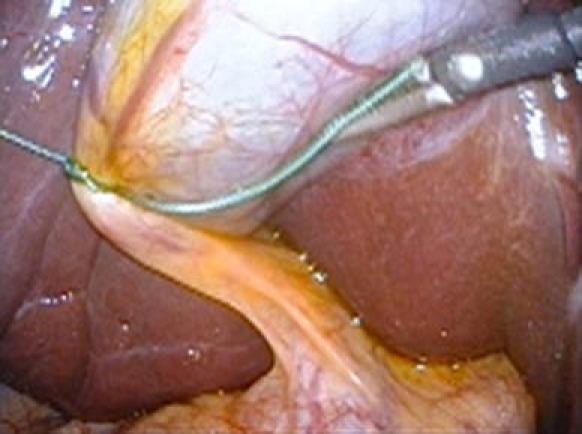
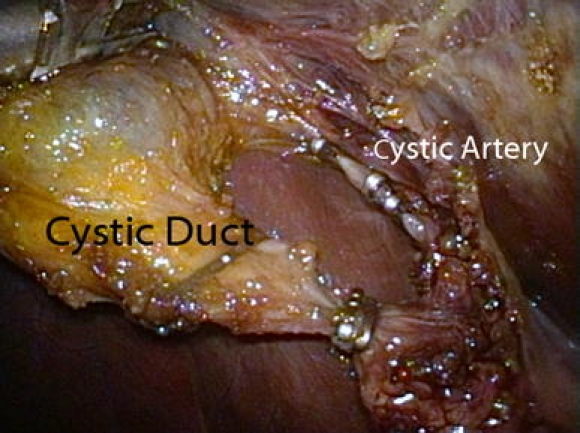
Methods: From January 2008 to March 2009, 100 patients with symptomatic gallbladder disease underwent SILC through a 1.5- to 2-cm umbilical incision using a two-port (5-mm) technique. For nearly all the patients, a 30 degrees angled scope was used. The gallbladder was retracted, with two or three sutures placed along the gallbladder. These sutures were either fixated internally or placed through the abdominal wall to obtain a critical view of Calot's triangle. The SILC procedure was performed using standard technique with 5-mm reticulating or conventional laparoscopic instruments. The cystic duct and artery were well visualized, clipped, and divided. Cholecystectomy was completed with electrocautery, and the specimen was retrieved through the umbilical incision.
Results: In this series, 80 women (85%) and 15 men (15%) with an average age of 33.8 years (range, 17-66 years) underwent SILC. Their mean BMI was 29.8 kg/m(2) (range, 17-42.5 kg/m(2)), and 39% of these patients had undergone previous abdominal surgery. The mean operative time was 50.8 min (range, 23-120 min). The mean estimated blood loss was 22.3 ml (range, 5-125 ml), and 5% of the patients had an intraoperative cholangiogram. There were no conversions of the SILC technique. A two-trocar technique was feasible for 87% of the patients. For the remaining patients, either a three-channel port or three individual trocars were required. A SILC technique was used for 5% of the patients to manage acute cholecystitis or gallstone pancreatitis.
Conclusion: The SILC technique with a two-trocar technique is safe, feasible, and reproducible. The operating times are reasonable and can be lessened with experience. Even complex cases can be managed with this technique. Excellent exposure of the critical view was obtained in all cases. The SILC procedure is becoming the standard of care for most of the authors' elective patients with gallbladder disease. Clinical trials are warranted before the SILC technique is adopted universally.
Figures



Similar articles
-
Learning curve of transumbilical single incision laparoscopic cholecystectomy (SILS): a preliminary study of 80 selected patients with benign gallbladder diseases.World J Surg. 2011 Sep;35(9):2092-101. doi: 10.1007/s00268-011-1144-1. World J Surg. 2011. PMID: 21660626
-
Single-incision laparoscopic cholecystectomy--can we afford that? Cost comparison of different surgical techniques.Pol Przegl Chir. 2014 Apr;86(4):177-80. doi: 10.2478/pjs-2014-0032. Pol Przegl Chir. 2014. PMID: 24988232
-
Single-incision laparoscopic cholecystectomy is associated with improved cosmesis scoring at the cost of significantly higher hernia rates: 1-year results of a prospective randomized, multicenter, single-blinded trial of traditional multiport laparoscopic cholecystectomy vs single-incision laparoscopic cholecystectomy.J Am Coll Surg. 2013 Jun;216(6):1037-47; discussion 1047-8. doi: 10.1016/j.jamcollsurg.2013.02.024. Epub 2013 Apr 23. J Am Coll Surg. 2013. PMID: 23619321 Clinical Trial.
-
Single-incision laparoscopic cholecystectomy: a surgeon's initial experience with 56 consecutive cases and a review of the literature.J Gastrointest Surg. 2010 Mar;14(3):506-10. doi: 10.1007/s11605-009-1116-z. Epub 2009 Dec 5. J Gastrointest Surg. 2010. PMID: 19967564 Review.
-
Single-incision versus conventional laparoscopic cholecystectomy in patients with uncomplicated gallbladder disease: a meta-analysis.Surg Laparosc Endosc Percutan Tech. 2012 Dec;22(6):487-97. doi: 10.1097/SLE.0b013e3182685d0a. Surg Laparosc Endosc Percutan Tech. 2012. PMID: 23238374 Review.
Cited by
-
Single-port cholecystectomy versus multi-port cholecystectomy: a prospective cohort study with 222 patients.World J Surg. 2013 May;37(5):991-8. doi: 10.1007/s00268-013-1946-4. World J Surg. 2013. PMID: 23435700 Clinical Trial.
-
Do height and weight affect the feasibility of single-incision laparoscopic cholecystectomy?Surg Endosc. 2015 Dec;29(12):3594-9. doi: 10.1007/s00464-015-4115-z. Epub 2015 Mar 11. Surg Endosc. 2015. PMID: 25759236
-
Differences in mental workload between traditional and single-incision laparoscopic procedures measured with a secondary task.Am J Surg. 2017 Feb;213(2):244-248. doi: 10.1016/j.amjsurg.2016.09.056. Epub 2016 Oct 8. Am J Surg. 2017. PMID: 27760704 Free PMC article.
-
Transumbilical single-incision laparoscopic distal pancreatectomy: primary experience and review of the English literature.World J Surg. 2014 May;38(5):1196-204. doi: 10.1007/s00268-013-2404-z. World J Surg. 2014. PMID: 24357245 Review.
-
Minimal invasive single-site surgery in colorectal procedures: Current state of the art.J Minim Access Surg. 2011 Jan;7(1):52-60. doi: 10.4103/0972-9941.72382. J Minim Access Surg. 2011. PMID: 21197243 Free PMC article.
References
-
- Cuschieri A (2005) Laparoscopic surgery: current status, issues, and future developments. Surgeon 3:125–130, 132–133, 135–138 - PubMed
-
- Cuschieri A. Minimal access surgery: the birth of a new era. J R Coll Surg Edinb. 1990;35:345–347. - PubMed
-
- Nagy AG, Poulin EC, Girotti MJ, Litwin DE, Mamazza J. History of laparoscopic surgery. Can J Surg. 1992;35:271–274. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
