

A simplified quantitative method for assessing keratoconjunctivitis sicca from the Sjögren's Syndrome International Registry
- PMID: 20035924
- PMCID: PMC3459675
- DOI: 10.1016/j.ajo.2009.09.013
A simplified quantitative method for assessing keratoconjunctivitis sicca from the Sjögren's Syndrome International Registry
Abstract
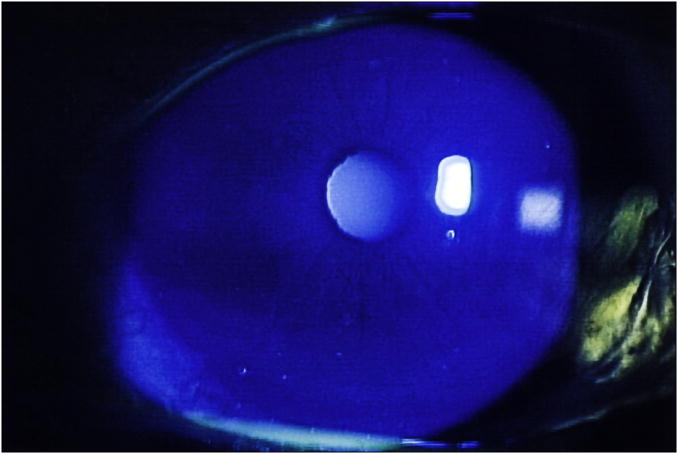
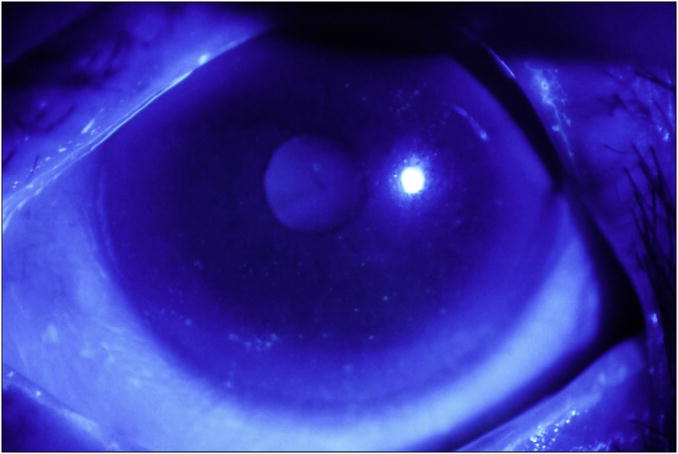
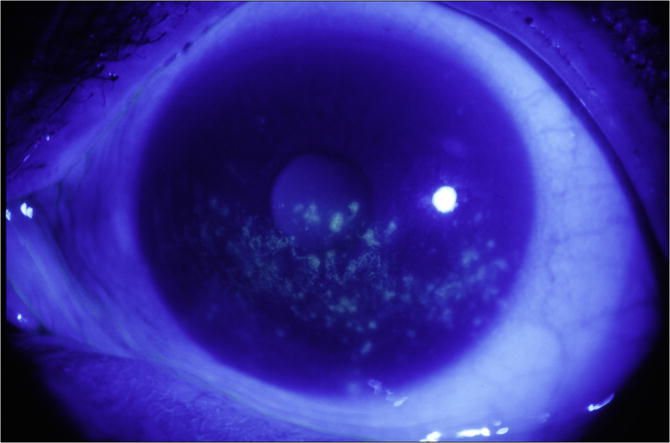
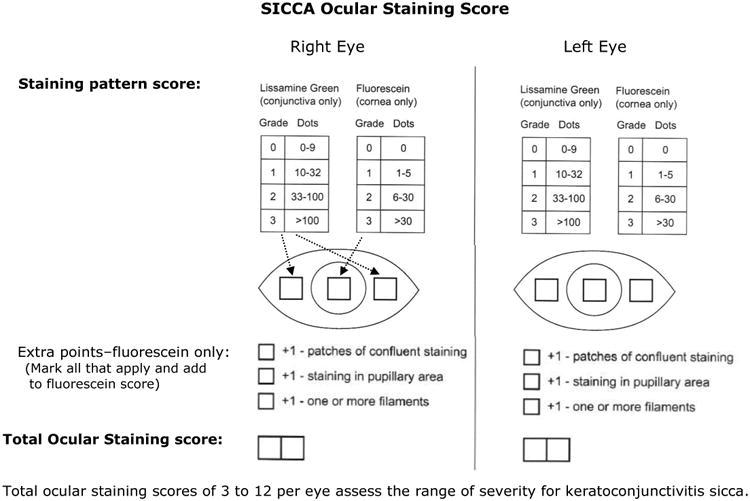
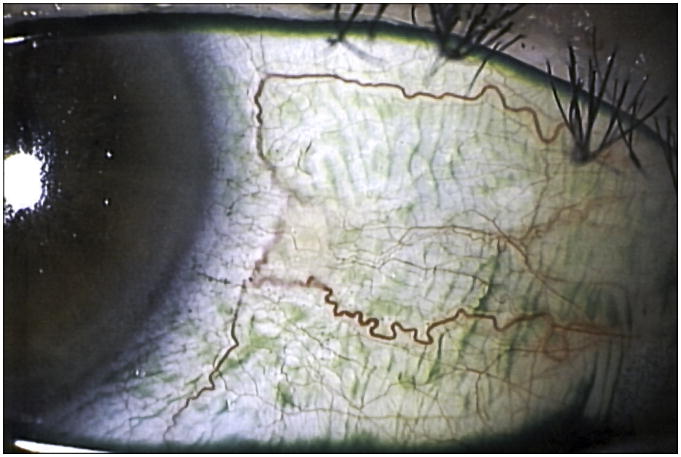
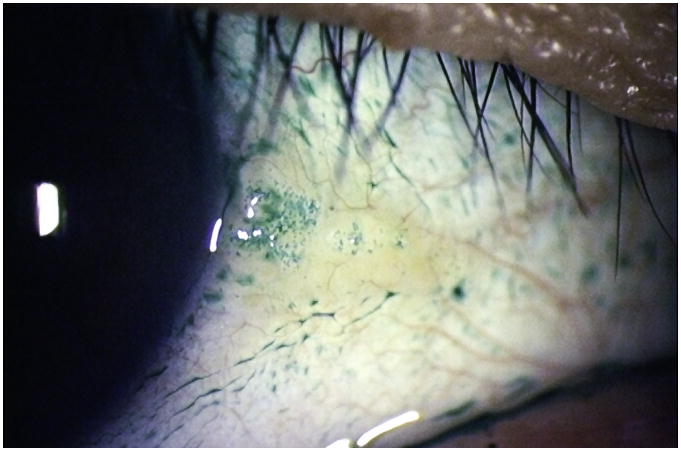
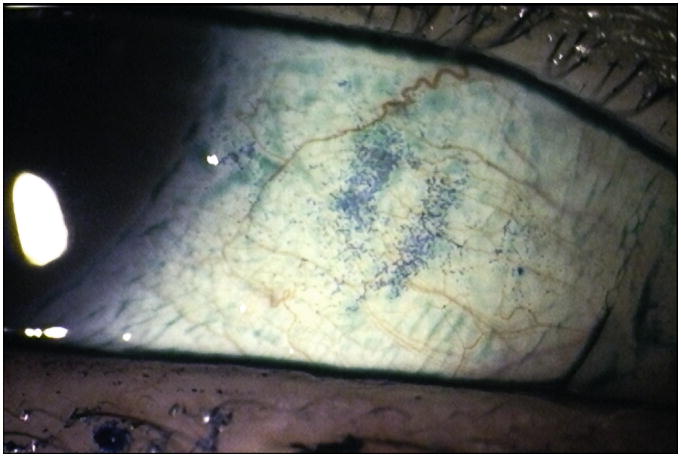
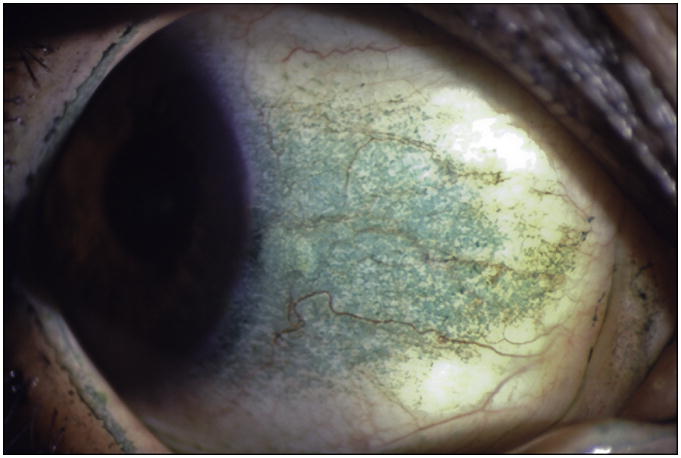
Purpose: To describe, apply, and test a new ocular grading system for assessing keratoconjunctivitis sicca (KCS) using lissamine green and fluorescein.
Design: Prospective, observational, multicenter cohort study.
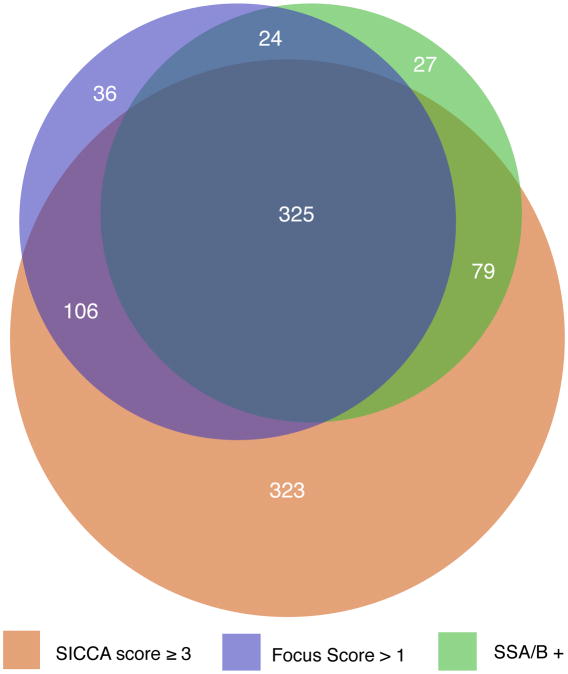
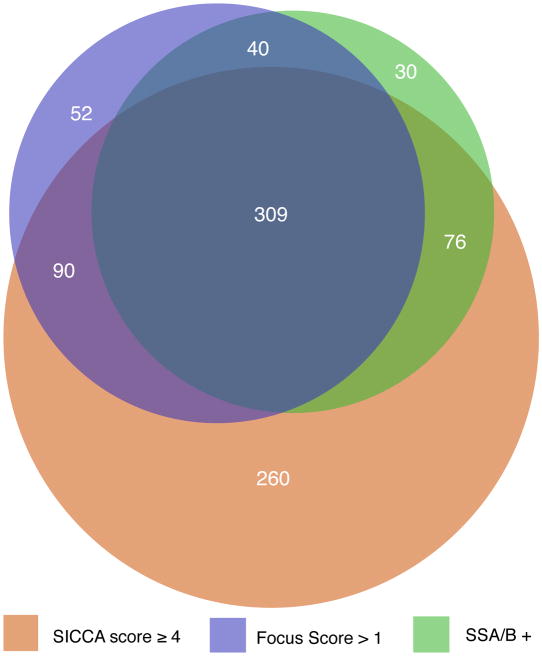
Methods: The National Institutes of Health-funded Sjögren's Syndrome International Registry (called Sjögren's International Collaborative Clinical Alliance [SICCA]) is developing standardized classification criteria for Sjögren syndrome (SS) and is creating a biospecimen bank for future research. Eight SICCA ophthalmologists developed a new quantitative ocular grading system (SICCA ocular staining score [OSS]), and we analyzed OSS distribution among the SICCA cohort and its association with other phenotypic characteristics of SS. The SICCA cohort includes participants ranging from possibly early SS to advanced disease. Procedures include sequenced unanesthetized Schirmer test, tear break-up time, ocular surface staining, and external eye examination at the slit lamp. Using statistical analyses and proportional Venn diagrams, we examined interrelationships between abnormal OSS (>or=3) and other characteristics of SS (labial salivary gland [LSG] biopsy with focal lymphocytic sialadenitis and focus score >1 positive anti-SS A antibodies, anti-SS B antibodies, or both).
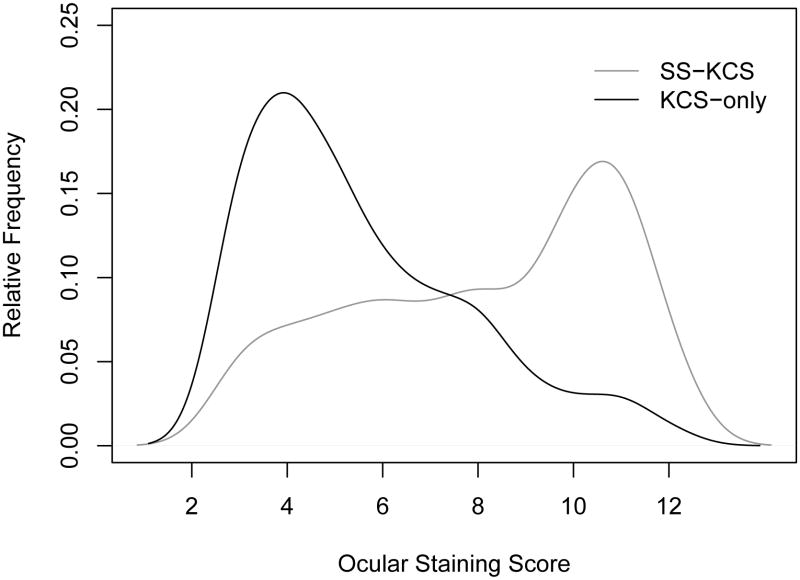
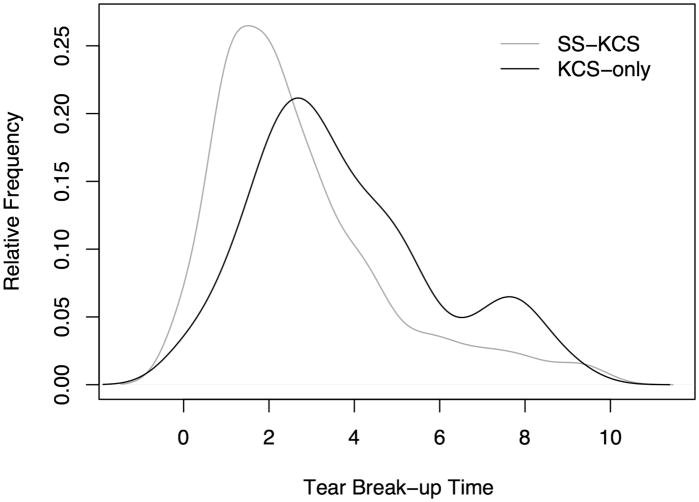
Results: Among 1208 participants, we found strong associations between abnormal OSS, positive serologic results, and positive LSG focus scores (P < .0001). Analysis of the overlapping relationships of these 3 measures defined a large group of participants who had KCS without other components of SS, representing a clinical entity distinct from the KCS associated with SS.
Conclusions: This new method for assessing KCS will become the means for diagnosing the ocular component of SS in future classification criteria. We find 2 forms of KCS whose causes may differ.
(c) 2010 Elsevier Inc. All rights reserved.
Figures
References
-
- Sjögren H. Zur Kenntis der Keratoconjunctivitis Sicca (Keratitis filiformis bei Hypofunktion der Tranendrusen) Acta Ophthalmol. 1933;(2):1–151.
-
- fluger P. Zur Ernahrung der cornea. Klin Monatsbl Augenheilkd. 1882;20:69–81.
-
- Holm S. Keratoconjunctivitis sicca and the sicca syndrome. Acta Ophthamologica. 1949;33(Suppl):1–230.
-
- van Bijsterveld OP. Diagnostic tests in the sicca syndrome. Arch Ophthal. 1969;82:10–14. - PubMed
-
- Norn MS. Lissamine green: Vital staining of cornea and conjunctiva. Acta Ophthalmologica. 1973;51:483–91. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
