

Insulin and hyperandrogenism in women with polycystic ovary syndrome
- PMID: 20036327
- PMCID: PMC3846536
- DOI: 10.1016/j.jsbmb.2009.12.010
Insulin and hyperandrogenism in women with polycystic ovary syndrome
Abstract
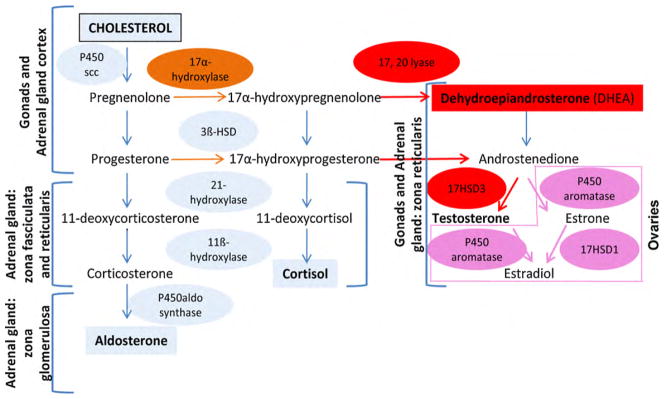
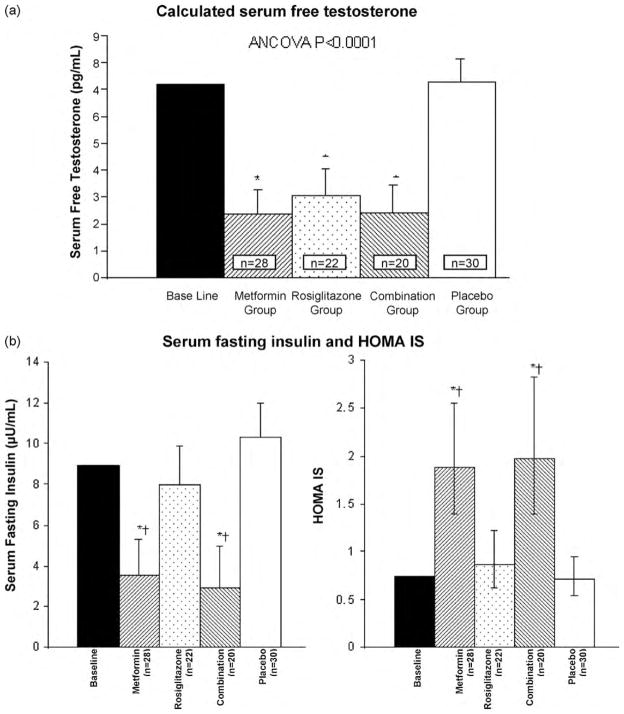
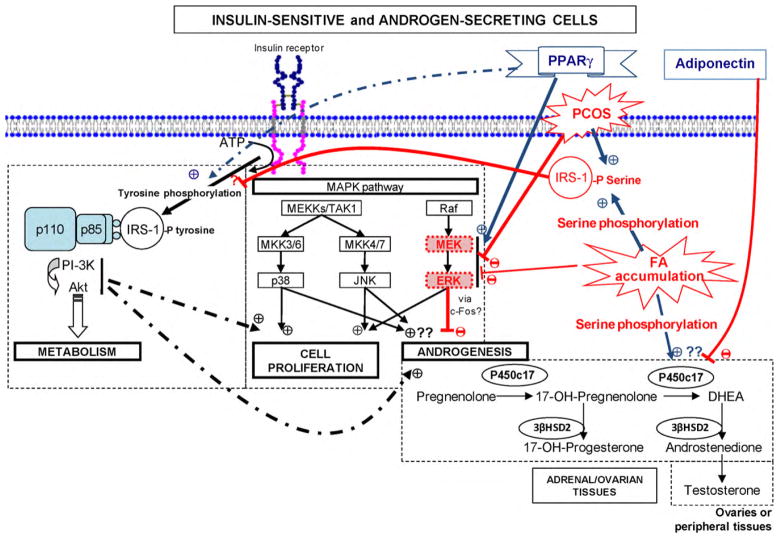
Polycystic ovary syndrome (PCOS) is a very common endocrine disorder characterized by chronic anovulation, clinical and/or biochemical hyperandrogenism, and/or polycystic ovaries. But most experts consider that hyperandrogenism is the main characteristic of PCOS. Several theories propose different mechanisms to explain PCOS manifestations: (1) a primary enzymatic default in the ovarian and/or adrenal steroidogenesis; (2) an impairment in gonadotropin releasing hormone (GnRH) secretion that promotes luteal hormone (LH) secretion; or (3) alterations in insulin actions that lead to insulin resistance with compensatory hyperinsulinemia. However, in the past 20 years there has been growing evidence supporting that defects in insulin actions or in the insulin signalling pathways are central in the pathogenesis of the syndrome. Indeed, most women with PCOS are metabolically insulin resistant, in part due to genetic predisposition and in part secondary to obesity. But some women with typical PCOS do not display insulin resistance, which supports the hypothesis of a genetic predisposition specific to PCOS that would be revealed by the development of insulin resistance and compensatory hyperinsulinemia in most, but not all, women with PCOS. However, these hypotheses are not yet appropriately confirmed, and more research is still needed to unravel the true pathogenesis underlying this syndrome. The present review thus aims at discussing new concepts and findings regarding insulin actions in PCOS women and how it is related to hyperandrogenemia.
Copyright © 2009 Elsevier Ltd. All rights reserved.
Figures
References
-
- Azziz R, Carmina E, Dewailly D, Diamanti-Kandarakis E, Escobar-Morreale HF, Futterweit W, Janssen OE, Legro RS, Norman RJ, Taylor AE, Witchel SF. The Androgen Excess and PCOS Society criteria for the polycystic ovary syndrome: the complete task force report. Fertil Steril. 2009;91(2):456–488. - PubMed
-
- Baillargeon JP. Use of insulin sensitizers in polycystic ovarian syndrome. Curr Opin Investig Drugs. 2005;6(10):1012–1022. - PubMed
-
- Zawadzki JK, Dunaif A. Current Issues in Endocrinology and Metabolism: Polycystic Ovary Syndrome. Blackwell Scientific Publications; Cambridge, MA: 1992. Diagnostic criteria for polycystic ovary syndrome: towards a rational approach; pp. 377–384.
-
- . Revised 2003 consensus on diagnostic criteria and long-term health risks related to polycystic ovary syndrome. Fertil Steril. 2004;81(1):19–25. - PubMed
-
- Azziz R, Carmina E, Dewailly D, Diamanti-Kandarakis E, Escobar-Morreale HF, Futterweit W, Janssen OE, Legro RS, Norman RJ, Taylor AE, Witchel SF. Positions statement: criteria for defining polycystic ovary syndrome as a predominantly hyperandrogenic syndrome: an Androgen Excess Society guideline. J Clin Endocrinol Metab. 2006;91(11):4237–4245. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
