

The pathophysiology of bronchiectasis
- PMID: 20037680
- PMCID: PMC2793069
- DOI: 10.2147/copd.s6133
The pathophysiology of bronchiectasis
Abstract
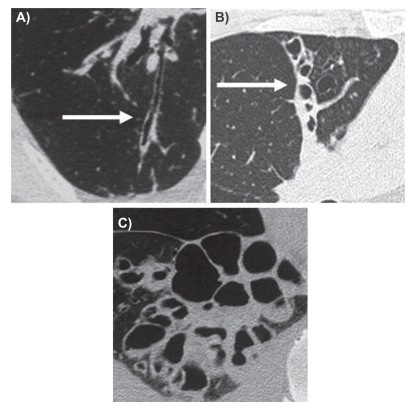
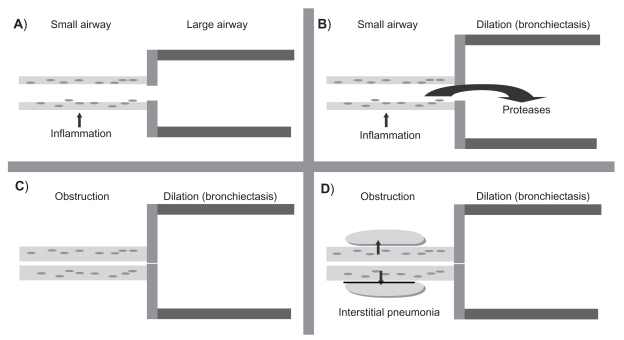
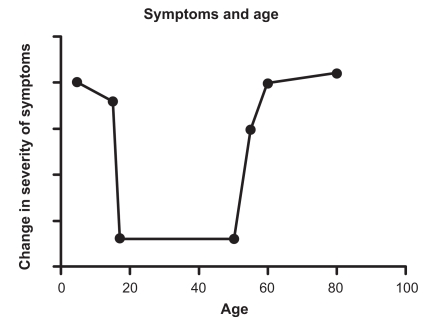
Bronchiectasis is defined by permanent and abnormal widening of the bronchi. This process occurs in the context of chronic airway infection and inflammation. It is usually diagnosed using computed tomography scanning to visualize the larger bronchi. Bronchiectasis is also characterized by mild to moderate airflow obstruction. This review will describe the pathophysiology of noncystic fibrosis bronchiectasis. Studies have demonstrated that the small airways in bronchiectasis are obstructed from an inflammatory infiltrate in the wall. As most of the bronchial tree is composed of small airways, the net effect is obstruction. The bronchial wall is typically thickened by an inflammatory infiltrate of lymphocytes and macrophages which may form lymphoid follicles. It has recently been demonstrated that patients with bronchiectasis have a progressive decline in lung function. There are a large number of etiologic risk factors associated with bronchiectasis. As there is generally a long-term retrospective history, it may be difficult to determine the exact role of such factors in the pathogenesis. Extremes of age and smoking/chronic obstructive pulmonary disease may be important considerations. There are a variety of different pathogens involved in bronchiectasis, but a common finding despite the presence of purulent sputum is failure to identify any pathogenic microorganisms. The bacterial flora appears to change with progression of disease.
Keywords: bronchiectasis; inflammation; obstructive lung disease; pathology; pathophysiology.
Figures
References
-
- Barker AF. Bronchiectasis. N Engl J Med. 2002;346:1383–1393. - PubMed
-
- King PT, Holdsworth SR, Freezer NJ, Villanueva E, Holmes PW. Characterisation of the onset and presenting clinical features of adult bronchiectasis. Respir Med. 2006;100:2183–2189. - PubMed
-
- McGuinness G, Naidich DP. CT of airways disease and bronchiectasis. Radiol Clin North Am. 2002;40:1–19. - PubMed
-
- Weycker D, Edelsberg J, Oster G, Tino G. Prevalence and economic burden of bronchiectasis. Clin Pulm Med. 2005;4:205–209.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
