

Combination flucytosine and high-dose fluconazole compared with fluconazole monotherapy for the treatment of cryptococcal meningitis: a randomized trial in Malawi
- PMID: 20038244
- PMCID: PMC2805957
- DOI: 10.1086/649861
Combination flucytosine and high-dose fluconazole compared with fluconazole monotherapy for the treatment of cryptococcal meningitis: a randomized trial in Malawi
Abstract
Background: Cryptococcal meningitis is a major cause of human immunodeficiency virus (HIV)-associated morbidity and mortality in Africa. Improved oral treatment regimens are needed because amphotericin B is neither available nor feasible in many centers. Fluconazole at a dosage of 1200 mg per day is more fungicidal than at a dosage of 800 mg per day, but mortality rates remain unacceptably high. Therefore, we examined the effect of adding oral flucytosine to fluconazole.
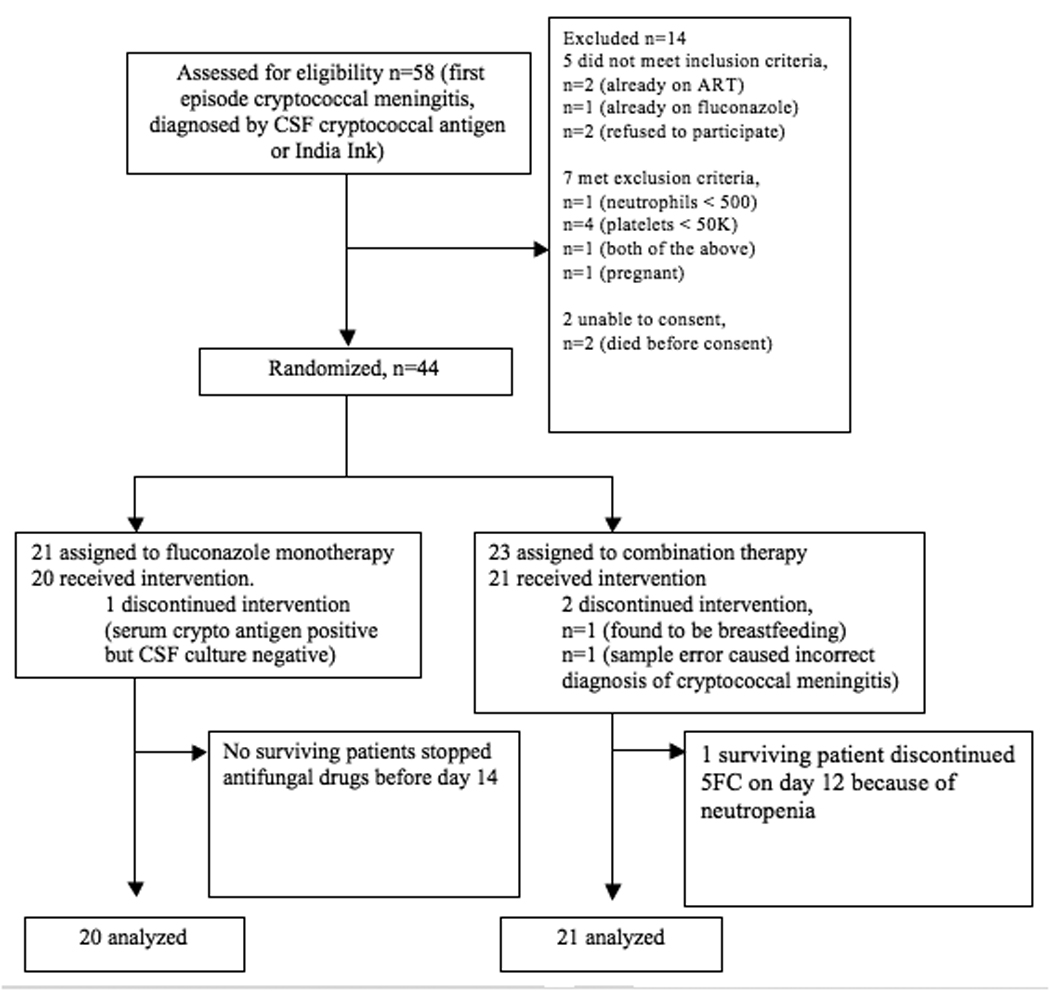
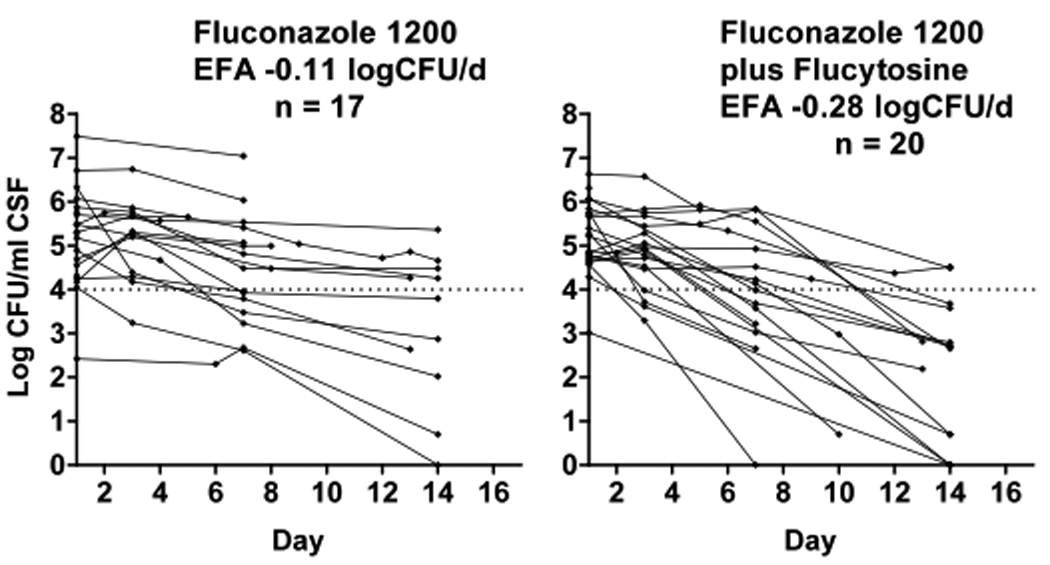
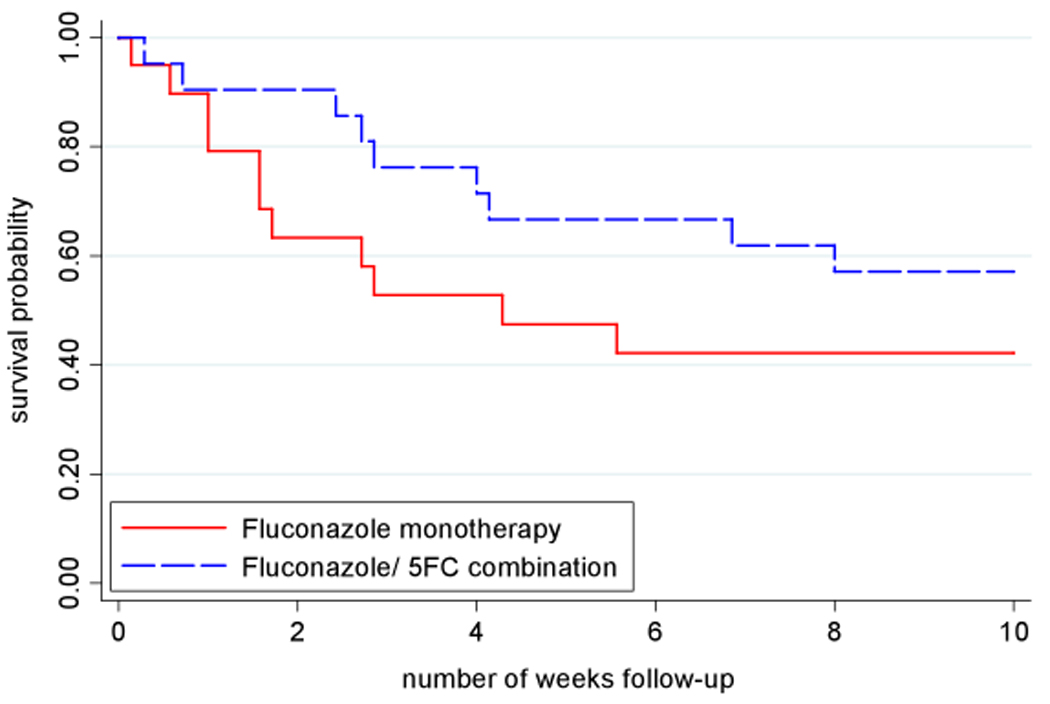
Methods: From 13 February through 2 December 2008, HIV-seropositive, antiretroviral-naive patients experiencing their first episode of cryptococcal meningitis were randomized to receive (1) 14 days of fluconazole (1200 mg per day) alone or (2) in combination with flucytosine (100 mg/kg per day) followed by fluconazole (800 mg per day), with both groups undergoing 10 weeks of follow-up. The primary end point was early fungicidal activity, derived from quantitative cerebrospinal fluid cultures on days 1, 3, 7, and 14. Secondary end points were safety and 2- and 10-week mortality.
Results: Forty-one patients were analyzed. Baseline mental status, cryptococcal burden, opening pressure, CD4(+) cell count, and HIV load were similar between groups. Combination therapy was more fungicidal than fluconazole alone (mean early fungicidal activity +/- standard deviation -0.28 +/- 0.17 log colony-forming units [CFU]/mL per day vs -0.11 +/- 0.09 log CFU/mL per day; P < .001). The combination arm had fewer deaths by 2 weeks (10% vs 37%) and 10 weeks (43% vs 58%). More patients had grade III or IV neutropenia with combination therapy (5 vs 1, within the first 2 weeks; P = .20), but there was no increase in infection-related adverse events.
Conclusions: The results suggest that optimal oral treatment for cryptococcal meningitis is high-dose fluconazole with flucytosine. Efforts are needed to increase availability of flucytosine in Africa. Clinical trials registration. isrctn.org Identifier: ISRCTN02725351.
Conflict of interest statement
Potential conflicts of interest: All authors: no conflicts
Figures
Comment in
-
Cryptococcosis in the developing world: an elephant in the parlor.Clin Infect Dis. 2010 Feb 1;50(3):345-6. doi: 10.1086/649862. Clin Infect Dis. 2010. PMID: 20038243 No abstract available.
References
-
- Gordon SB, Walsh AL, Chaponda M, et al. Bacterial meningitis in Malawian adults: pneumococcal disease is common, severe, and seasonal. Clinical Infectious Diseases. 2000;31:53–57. - PubMed
-
- Hakim JG, Gangaidzo IT, Heyderman RS, et al. Impact of HIV infection on meningitis in Harare, Zimbabwe: a prospective study of 406 predominantly adult patients. AIDS. 2000;14:1401–1407. - PubMed
-
- Holmes CB, Losina E, Walensky RP, Yazdanpanah Y, Freedberg KA. Review of human immunodeficiency virus type 1-related opportunistic infections in sub-Saharan Africa. Clin Infect Dis. 2003;36:652–662. - PubMed
-
- Corbett EL, Churchyard GJ, Charalambos S, et al. Morbidity and mortality in South African gold miners: impact of untreated disease due to human immunodeficiency virus. Clin Infect Dis. 2002;34:1251–1258. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
