

Clinical pharmacodynamics of cefepime in patients infected with Pseudomonas aeruginosa
- PMID: 20038614
- PMCID: PMC2825990
- DOI: 10.1128/AAC.01183-09
Clinical pharmacodynamics of cefepime in patients infected with Pseudomonas aeruginosa
Abstract
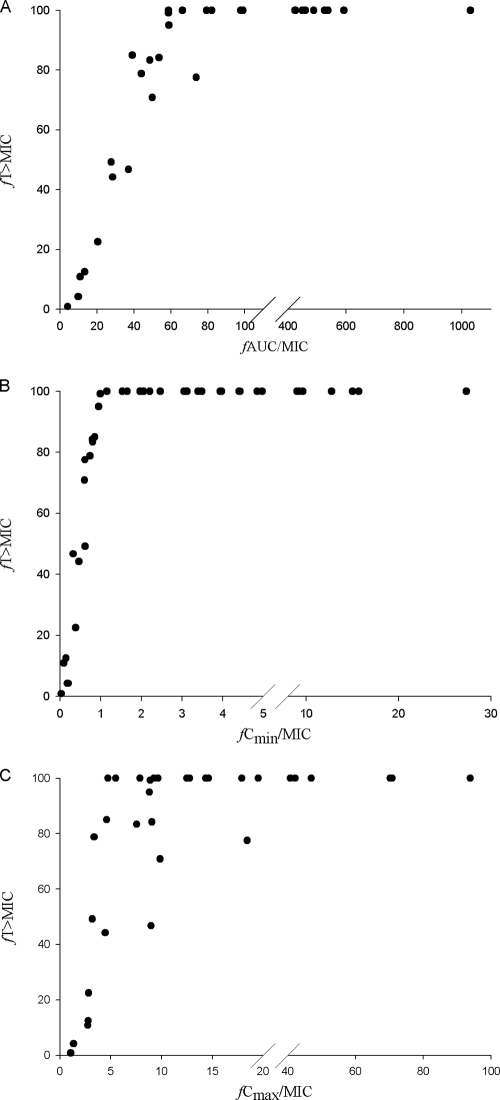
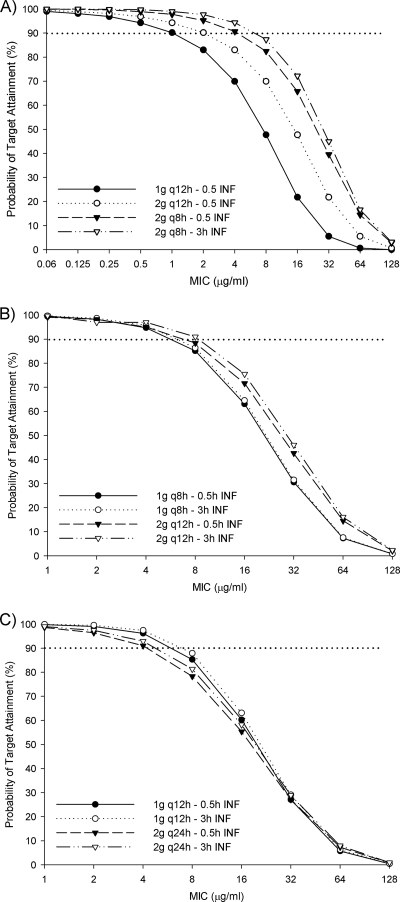
We evaluated cefepime exposures in patients infected with Pseudomonas aeruginosa to identify the pharmacodynamic relationship predictive of microbiological response. Patients with non-urinary tract P. aeruginosa infections and treated with cefepime were included. Free cefepime exposures were estimated by using a validated population pharmacokinetic model. P. aeruginosa MICs were determined by Etest and pharmacodynamic indices (the percentage of the dosing interval that the free drug concentration remains above the MIC of the infecting organism [fT > MIC], the ratio of the minimum concentration of free drug to the MIC [fC(min)/MIC], and the ratio of the area under the concentration-time curve for free drug to the MIC [fAUC/MIC]) were calculated for each patient. Classification and regression tree analysis was used to partition the pharmacodynamic parameters for prediction of the microbiological response. Monte Carlo simulation was utilized to determine the optimal dosing regimens needed to achieve the pharmacodynamic target. Fifty-six patients with pneumonia (66.1%), skin and skin structure infections (SSSIs) (25%), and bacteremia (8.9%) were included. Twenty-four (42.9%) patients failed cefepime therapy. The MICs ranged from 0.75 to 96 microg/ml, resulting in median fT > MIC, fC(m)(in)/MIC, and fAUC/MIC exposures of 100% (range, 0.8 to 100%), 4.3 (range, 0.1 to 27.3), and 206.2 (range, 4.2 to 1,028.7), respectively. Microbiological failure was associated with an fT > MIC of < or =60% (77.8% failed cefepime therapy when fT > MIC was < or =60%, whereas 36.2% failed cefepime therapy when fT > MIC was >60%; P = 0.013). A similar fT > MIC target of < or =63.9% (P = 0.009) was identified when skin and skin structure infections were excluded. While controlling for the SSSI source (odds ratio [OR], 0.18 [95% confidence interval, 0.03 to 1.19]; P = 0.07) and combination therapy (OR, 2.15 [95% confidence interval, 0.59 to 7.88]; P = 0.25), patients with fT > MIC values of < or =60% were 8.1 times (95% confidence interval, 1.2 to 55.6 times) more likely to experience a poor microbiological response. Cefepime doses of at least 2 g every 8 h are required to achieve this target against CLSI-defined susceptible P. aeruginosa organisms in patients with normal renal function. In patients with non-urinary tract infections caused by P. aeruginosa, achievement of cefepime exposures of >60% fT > MIC will minimize the possibility of a poor microbiological response.
Figures
Similar articles
-
Cefepime pharmacodynamics in patients with extended spectrum beta-lactamase (ESBL) and non-ESBL infections.J Infect. 2007 May;54(5):463-8. doi: 10.1016/j.jinf.2006.09.004. Epub 2006 Oct 24. J Infect. 2007. PMID: 17067681
-
Clinical pharmacodynamics of antipseudomonal cephalosporins in patients with ventilator-associated pneumonia.Antimicrob Agents Chemother. 2014;58(3):1359-64. doi: 10.1128/AAC.01463-13. Epub 2013 Dec 16. Antimicrob Agents Chemother. 2014. PMID: 24342637 Free PMC article.
-
Pharmacokinetic-pharmacodynamic rationale for cefepime dosing regimens in intensive care units.J Antimicrob Chemother. 2006 Nov;58(5):987-93. doi: 10.1093/jac/dkl349. Epub 2006 Aug 30. J Antimicrob Chemother. 2006. PMID: 16943209
-
Pharmacodynamic considerations in the treatment of moderate to severe pseudomonal infections with cefepime.J Antimicrob Chemother. 2002 Mar;49(3):445-53. doi: 10.1093/jac/49.3.445. J Antimicrob Chemother. 2002. PMID: 11864944 Review.
-
The Pharmacodynamics of Prolonged Infusion β-Lactams for the Treatment of Pseudomonas aeruginosa Infections: A Systematic Review.Clin Ther. 2019 Nov;41(11):2397-2415.e8. doi: 10.1016/j.clinthera.2019.09.010. Epub 2019 Nov 1. Clin Ther. 2019. PMID: 31679822
Cited by
-
Efficacy of human simulated exposures of ceftaroline against phenotypically diverse Enterobacteriaceae isolates.Antimicrob Agents Chemother. 2012 May;56(5):2576-80. doi: 10.1128/AAC.06416-11. Epub 2012 Feb 13. Antimicrob Agents Chemother. 2012. PMID: 22330908 Free PMC article.
-
Intrapulmonary Pharmacokinetic Modeling and Simulation of Cefiderocol, a Parenteral Siderophore Cephalosporin, in Patients With Pneumonia and Healthy Subjects.J Clin Pharmacol. 2022 May;62(5):670-680. doi: 10.1002/jcph.1986. Epub 2022 Feb 26. J Clin Pharmacol. 2022. PMID: 34648652 Free PMC article.
-
Broad-spectrum β-lactams in obese non-critically ill patients.Nutr Diabetes. 2014 Jun 23;4(6):e119. doi: 10.1038/nutd.2014.15. Nutr Diabetes. 2014. PMID: 24956136 Free PMC article.
-
In vivo activities of simulated human doses of cefepime and cefepime-AAI101 against multidrug-resistant Gram-negative Enterobacteriaceae.Antimicrob Agents Chemother. 2015 May;59(5):2688-94. doi: 10.1128/AAC.00033-15. Epub 2015 Feb 23. Antimicrob Agents Chemother. 2015. PMID: 25712356 Free PMC article.
-
Elevated MICs of Susceptible Antipseudomonal Cephalosporins in Non-Carbapenemase-Producing, Carbapenem-Resistant Pseudomonas aeruginosa: Implications for Dose Optimization.Antimicrob Agents Chemother. 2021 Oct 18;65(11):e0120421. doi: 10.1128/AAC.01204-21. Epub 2021 Aug 16. Antimicrob Agents Chemother. 2021. PMID: 34398670 Free PMC article.
References
-
- American Thoracic Society and Infectious Diseases Society of America. 2005. Guidelines for the management of adults with hospital-acquired, ventilator-associated, and healthcare-associated pneumonia. Am. J. Respir. Crit. Care Med. 171:388-416. - PubMed
-
- Charlson, M. E., P. Pompei, K. L. Ales, and C. R. MacKenzie. 1987. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J. Chronic Dis. 40:373-383. - PubMed
-
- Clinical and Laboratory Standards Institute. 2008. Methods for dilution antimicrobial susceptibility tests for bacteria that grow aerobically; approved standard, 8th ed. CLSI publication M07-A8. Clinical and Laboratory Standards Institute, Wayne, PA.
-
- Craig, W. A. 1998. Pharmacokinetic/pharmacodynamic parameters: rationale for antibacterial dosing of mice and men. Clin. Infect. Dis. 26:1-10. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
