

Pharmacokinetics of antituberculosis drugs in pulmonary tuberculosis patients with type 2 diabetes
- PMID: 20038625
- PMCID: PMC2825975
- DOI: 10.1128/AAC.00447-09
Pharmacokinetics of antituberculosis drugs in pulmonary tuberculosis patients with type 2 diabetes
Abstract
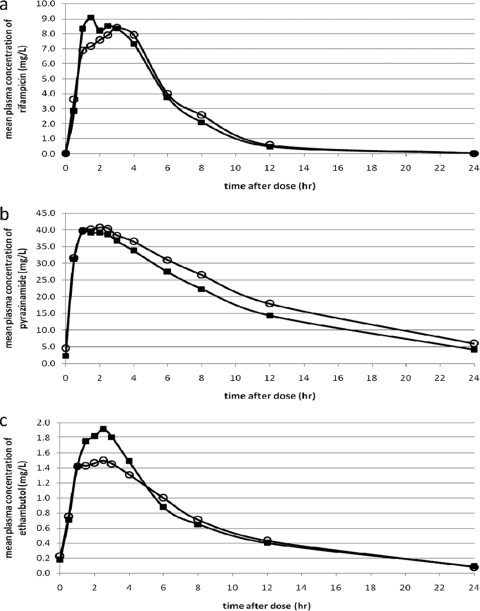
Altered pharmacokinetics of antituberculosis drugs may contribute to an increased risk of tuberculosis treatment failure for diabetic patients. We previously found that rifampin exposure was 2-fold lower in diabetic than in nondiabetic tuberculosis patients during the continuation phase of treatment. We now examined the influence of diabetes on the pharmacokinetics of antituberculosis drugs in the intensive phase of tuberculosis treatment, and we evaluated the effect of glycemic control. For this purpose, 18 diabetic and 18 gender- and body weight-matched nondiabetic tuberculosis patients were included in an Indonesian setting. Intensive pharmacokinetic sampling was performed for rifampin, pyrazinamide, and ethambutol at steady state. The bioavailability of rifampin was determined by comparing rifampin exposure after oral versus intravenous administration. Pharmacokinetic assessments were repeated for 10 diabetic tuberculosis patients after glycemic control. No differences in the areas under the concentration-time curves of the drugs in plasma from 0 to 24 h postdose (AUC(0-24)), the maximum concentrations of the drugs in plasma (C(max)), the times to C(max) (T(max)), and the half-lives of rifampin, pyrazinamide, and ethambutol were found between diabetic and nondiabetic tuberculosis patients in the intensive phase of tuberculosis treatment. For rifampin, oral bioavailability and metabolism were similar in diabetic and nondiabetic patients. The pharmacokinetic parameters of antituberculosis drugs were not correlated with blood glucose levels or glucose control. We conclude that diabetes does not alter the pharmacokinetics of antituberculosis drugs during the intensive phase of tuberculosis treatment. The reduced exposure to rifampin of diabetic patients in the continuation phase may be due to increased body weight and possible differences in hepatic induction. Further research is needed to determine the cause of increased tuberculosis treatment failure among diabetic patients.
Figures

Similar articles
-
Optimizing treatment outcome of first-line anti-tuberculosis drugs: the role of therapeutic drug monitoring.Eur J Clin Pharmacol. 2016 Aug;72(8):905-16. doi: 10.1007/s00228-016-2083-4. Epub 2016 Jun 15. Eur J Clin Pharmacol. 2016. PMID: 27305904 Review.
-
Plasma concentrations of isoniazid and rifampin are decreased in adult pulmonary tuberculosis patients with diabetes mellitus.Antimicrob Agents Chemother. 2013 Nov;57(11):5740-2. doi: 10.1128/AAC.01345-13. Epub 2013 Aug 26. Antimicrob Agents Chemother. 2013. PMID: 23979746 Free PMC article.
-
Isoniazid, rifampin, ethambutol, and pyrazinamide pharmacokinetics and treatment outcomes among a predominantly HIV-infected cohort of adults with tuberculosis from Botswana.Clin Infect Dis. 2009 Jun 15;48(12):1685-94. doi: 10.1086/599040. Clin Infect Dis. 2009. PMID: 19432554 Free PMC article.
-
Pharmacokinetics of Rifampin, Isoniazid, Pyrazinamide, and Ethambutol in Infants Dosed According to Revised WHO-Recommended Treatment Guidelines.Antimicrob Agents Chemother. 2016 Mar 25;60(4):2171-9. doi: 10.1128/AAC.02600-15. Print 2016 Apr. Antimicrob Agents Chemother. 2016. PMID: 26810651 Free PMC article. Clinical Trial.
-
Present status of chemotherapy for tuberculosis.Rev Infect Dis. 1989 Mar-Apr;11 Suppl 2:S347-52. doi: 10.1093/clinids/11.supplement_2.s347. Rev Infect Dis. 1989. PMID: 2652251 Review.
Cited by
-
Optimizing treatment outcome of first-line anti-tuberculosis drugs: the role of therapeutic drug monitoring.Eur J Clin Pharmacol. 2016 Aug;72(8):905-16. doi: 10.1007/s00228-016-2083-4. Epub 2016 Jun 15. Eur J Clin Pharmacol. 2016. PMID: 27305904 Review.
-
The challenge of new drug discovery for tuberculosis.Nature. 2011 Jan 27;469(7331):483-90. doi: 10.1038/nature09657. Nature. 2011. PMID: 21270886 Review.
-
Impact of diabetes on the natural history of tuberculosis.Diabetes Res Clin Pract. 2014 Nov;106(2):191-9. doi: 10.1016/j.diabres.2014.06.011. Epub 2014 Jul 14. Diabetes Res Clin Pract. 2014. PMID: 25082309 Free PMC article. Review.
-
Clinical management of concurrent diabetes and tuberculosis and the implications for patient services.Lancet Diabetes Endocrinol. 2014 Sep;2(9):740-53. doi: 10.1016/S2213-8587(14)70110-X. Lancet Diabetes Endocrinol. 2014. PMID: 25194887 Free PMC article. Review.
-
State of the art of real-life concentration monitoring of rifampicin and its implementation contextualized in resource-limited settings: the Tanzanian case.JAC Antimicrob Resist. 2024 Nov 14;6(6):dlae182. doi: 10.1093/jacamr/dlae182. eCollection 2024 Dec. JAC Antimicrob Resist. 2024. PMID: 39544428 Free PMC article. Review.
References
-
- Alisjahbana, B., R. van Crevel, E. Sahiratmadja, M. Heijer, A. Maya, E. Istriana, H. Danusantoso, T. H. Ottenhoff, R. H. Nelwan, and J. W. van der Meer. 2006. Diabetes mellitus is strongly associated with tuberculosis in Indonesia. Int. J. Tuberc. Lung Dis. 10:696-699. - PubMed
-
- Alisjahbana, B., E. Sahiratmadja, E. J. Nelwan, A. M. Purwa, Y. Ahmad, T. H. Ottenhoff, R. H. Nelwan, I. Parwati, J. W. van der Meer, and R. van Crevel. 2007. The effect of type 2 diabetes mellitus on the presentation and treatment response of pulmonary tuberculosis. Clin. Infect. Dis. 45:428-435. - PubMed
-
- Boucot, K. R. 1957. Diabetes mellitus and pulmonary tuberculosis. J. Chronic Dis. 6:256-279. - PubMed
-
- Burman, W. J., K. Gallicano, and C. A. Peloquin. 2001. Comparative pharmacokinetics and pharmacodynamics of the rifamycin antibacterials. Clin. Pharmacokinet. 40:327-341. - PubMed
-
- Fromm, M. F., D. Busse, H. K. Kroemer, and M. Eichelbaum. 1996. Differential induction of prehepatic and hepatic metabolism of verapamil by rifampin. Hepatology 24:796-801. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
