

In situ expression of cagA and risk of gastroduodenal disease in Helicobacter pylori-infected children
- PMID: 20038850
- PMCID: PMC2824336
- DOI: 10.1097/MPG.0b013e3181bab326
In situ expression of cagA and risk of gastroduodenal disease in Helicobacter pylori-infected children
Abstract
Background and aim: Gastroduodenal disease is more common among adults and children with cagA+ Helicobacter pylori infection, but disease severity varies among those infected with cagA+ strains. We examined whether cagA in situ expression can predict disease manifestations among H pylori-infected children.
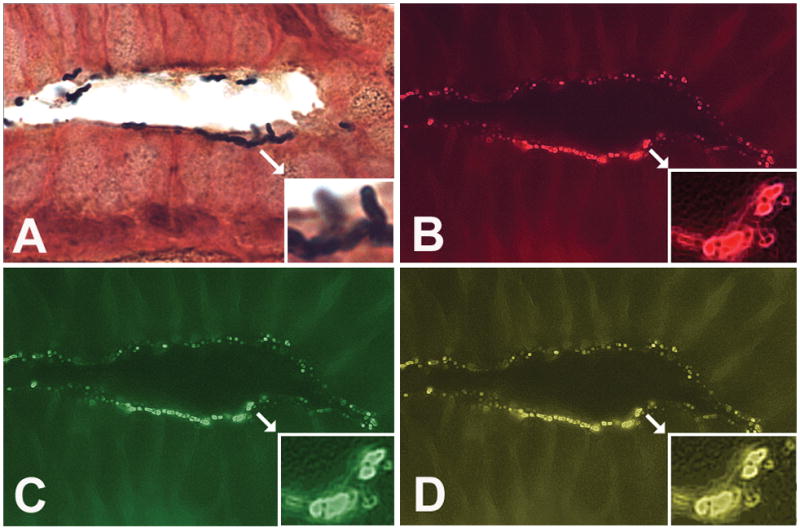
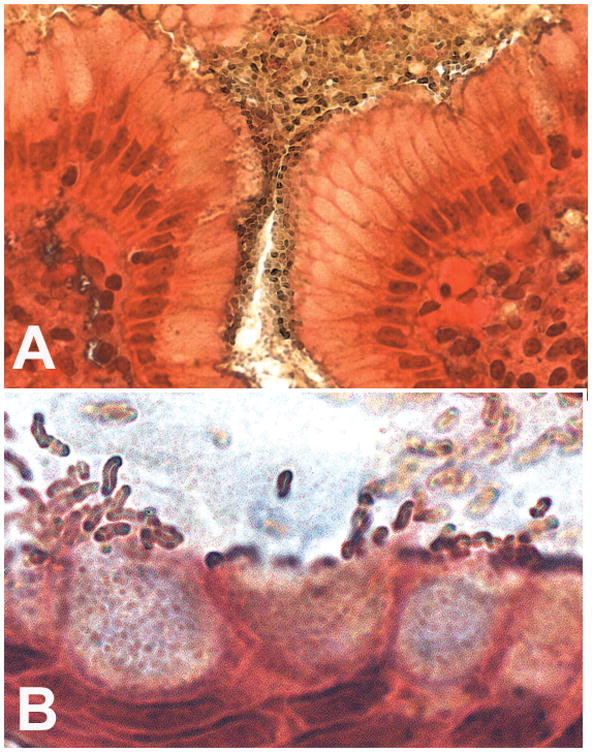
Patients and methods: Fifty-one children were selected from 805 patients with abdominal symptoms who underwent esophagogastroduodenoscopy with gastric biopsies. Endoscopic and histologic gastritis were scored and H pylori colonization was quantified by Genta stain and in situ hybridization expression of 16S rRNA and cagA.
Results: Endoscopy was either normal (n = 14) or demonstrated nodularity (n = 18), gastric ulcer (n = 8) or duodenal ulcer (n = 11). H pylori was present in 7, 18, 6, and 10 children, respectively. Expression of 16S rRNA and cagA were significantly higher in children with ulcer compared with normal children. The fraction of H pylori bacteria expressing cagA in situ was higher in children with ulcer compared to those with endoscopic nodularity (P < 0.05).
Conclusions: Thus, cagA in situ expression is increased in H pylori-infected children with peptic ulcers and may play a role in the pathogenesis of peptic ulcer disease during childhood. Determination of in situ expression of cagA complements traditional isolation and in vitro testing of single-colony isolates.
Conflict of interest statement
No potential, perceived, or real conflict of interest exist
Figures
Similar articles
-
Reciprocal impact of host factors and Helicobacter pylori genotypes on gastric diseases.World J Gastroenterol. 2015 Aug 21;21(31):9317-27. doi: 10.3748/wjg.v21.i31.9317. World J Gastroenterol. 2015. PMID: 26309357 Free PMC article.
-
Study of the cytoxin-associated gene a (CagA gene) in Helicobacter pylori using gastric biopsies of Iraqi patients.Saudi J Gastroenterol. 2013 Mar-Apr;19(2):69-74. doi: 10.4103/1319-3767.108474. Saudi J Gastroenterol. 2013. PMID: 23481132 Free PMC article.
-
Presence of the cagA gene in the majority of Helicobacter pylori strains is independent of whether the individual has duodenal ulcer or asymptomatic gastritis.Helicobacter. 1996 Jun;1(2):107-11. doi: 10.1111/j.1523-5378.1996.tb00019.x. Helicobacter. 1996. PMID: 9398887
-
H. pylori and cagA: relationships with gastric cancer, duodenal ulcer, and reflux esophagitis and its complications.Helicobacter. 1998 Sep;3(3):145-51. doi: 10.1046/j.1523-5378.1998.08031.x. Helicobacter. 1998. PMID: 9731983 Review.
-
Geographic differences and the role of cagA gene in gastroduodenal diseases associated with Helicobacter pylori infection.Rev Esp Enferm Dig. 2001 Jul;93(7):471-80. Rev Esp Enferm Dig. 2001. PMID: 11685943 Review. English, Spanish.
Cited by
-
Type I and type II Helicobacter pylori infection status and their impact on gastrin and pepsinogen level in a gastric cancer prevalent area.World J Gastroenterol. 2020 Jul 7;26(25):3673-3685. doi: 10.3748/wjg.v26.i25.3673. World J Gastroenterol. 2020. PMID: 32742135 Free PMC article.
-
The role of microbiomes in gastrointestinal cancers: new insights.Front Oncol. 2024 Feb 1;13:1344328. doi: 10.3389/fonc.2023.1344328. eCollection 2023. Front Oncol. 2024. PMID: 38361500 Free PMC article. Review.
-
The high expression of glial cell line-derived neurotrophic factor receptor alpha Ⅱ (GFRA2) as a predictor of poor prognosis in gastric cancer patients: A survival and regression analysis approach.Heliyon. 2023 Jul 17;9(7):e18291. doi: 10.1016/j.heliyon.2023.e18291. eCollection 2023 Jul. Heliyon. 2023. PMID: 37519699 Free PMC article.
-
Gastric cancer: a comprehensive review of current and future treatment strategies.Cancer Metastasis Rev. 2020 Dec;39(4):1179-1203. doi: 10.1007/s10555-020-09925-3. Epub 2020 Sep 7. Cancer Metastasis Rev. 2020. PMID: 32894370 Free PMC article. Review.
-
Role of mucin Lewis status in resistance to Helicobacter pylori infection in pediatric patients.Helicobacter. 2010 Aug;15(4):251-8. doi: 10.1111/j.1523-5378.2010.00765.x. Helicobacter. 2010. PMID: 20633185 Free PMC article.
References
-
- Atherton JC. The pathogenesis of Helicobacter pylori-induced gastro-duodenal diseases. Annu Rev Pathol. 2006;1:63–96. - PubMed
-
- Sherman P, Czinn S, Drumm B, Gottrand F, Kawakami E, et al. Helicobacter pylori infection in children and adolescents: Working Group Report of the First World Congress of Pediatric Gastroenterology, Hepatology, and Nutrition. J Pediatr Gastroenterol Nutr. 2002;35:S128–S133. - PubMed
-
- Go MF, Graham DY. How does Helicobacter pylori cause duodenal ulcer disease: the bug, the host, or both? J Gastroenterol Hepatol. 1994;9 (Suppl 1):S8–10. - PubMed
-
- Atherton JC, Tham KT, Peek RM, Jr, Cover TL. Density of Helicobacter pylori infection in vivo as assessed by quantitative culture and histology. J Infect Dis. 1996;174:552–556. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
