

Acute lung injury in patients with traumatic injuries: utility of a panel of biomarkers for diagnosis and pathogenesis
- PMID: 20038857
- PMCID: PMC3347639
- DOI: 10.1097/TA.0b013e3181c40728
Acute lung injury in patients with traumatic injuries: utility of a panel of biomarkers for diagnosis and pathogenesis
Abstract
Background: The diagnosis of acute lung injury (ALI) is based on a consensus clinical definition. Despite the simplicity of this definition, ALI remains underdiagnosed and undertreated. Severe trauma is a well-described cause of ALI that represents a relatively homogeneous subset of patients with ALI. The aims of this study were to develop a panel of plasma biomarkers to facilitate diagnosis of trauma-induced ALI and to enhance our understanding of the pathogenesis of human ALI.
Methods: A retrospective nested case control of 192 patients admitted to the trauma intensive care unit at a university hospital between 2002 and 2006. We compared 107 patients with ALI to 85 patients without ALI. Plasma was collected within 72 hours of intensive care unit admission. Twenty-one plasma biomarkers were measured in duplicate in each plasma sample.
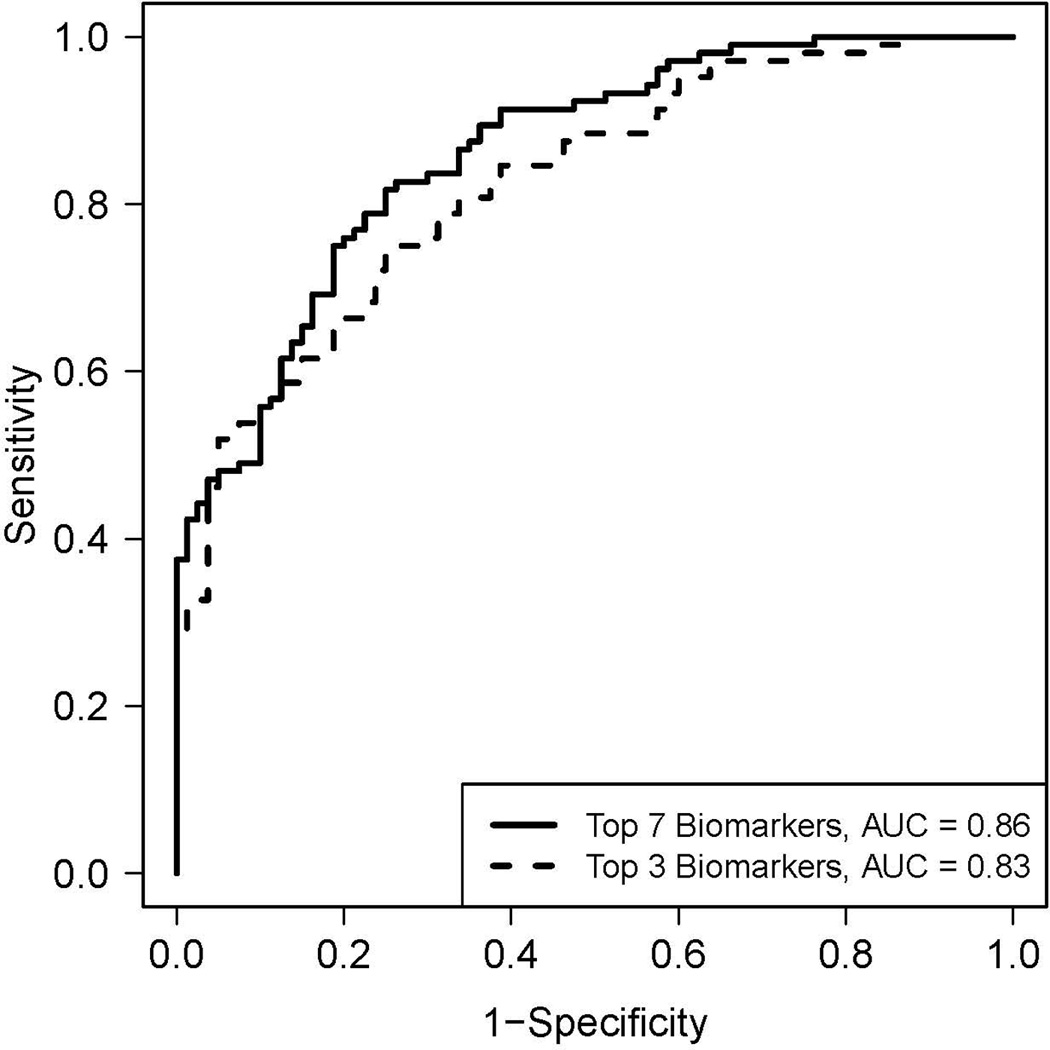
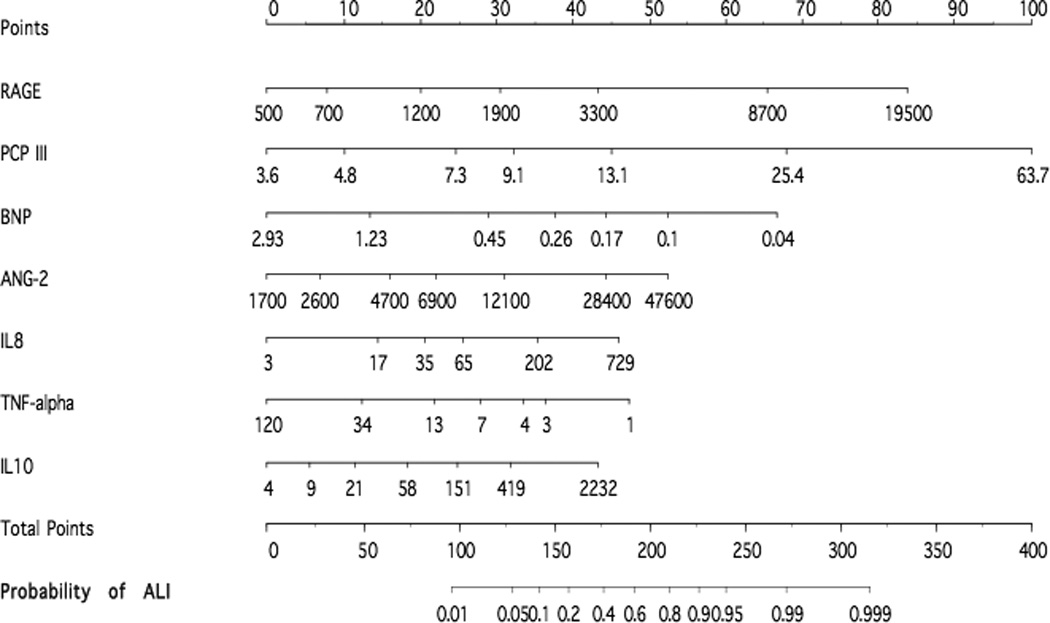
Results: Patients with ALI had higher severity of illness scores, more days of mechanical ventilation, longer hospital stays, and higher mortality versus controls. Seven biomarkers (receptor for advanced glycation end products, procollagen peptide III, brain natriuretic peptide, angiopoietin-2, interleukin-10, tumor necrosis factor alpha, and interleukin-8) had a high diagnostic accuracy as reflected by the area under the receiver operating characteristic curve of 0.86 (95% confidence interval, 0.82-0.92) in differentiating ALI from controls.
Conclusions: A model using seven plasma biomarkers had a high diagnostic accuracy in differentiating patients with trauma-induced ALI from trauma patients without ALI. In addition, use of a panel of biomarkers provides insight into the likely importance of alveolar epithelial injury in the pathogenesis of early ALI.
Figures
References
-
- Stapleton RD, Wang BM, Hudson LD, Rubenfeld GD, Caldwell ES, Steinberg KP. Causes and timing of death in patients with ARDS. Chest. 2005 Aug;128(2):525–532. - PubMed
-
- Eisner M, Thompson T, Hudson L, et al. Efficacy of low tidal volume ventilation in patients with different clinical risk factors for acute lung injury and the acute respiratory distress syndrome. Am J Respir Crit Care Med. 2001;164:231–236. - PubMed
-
- Estenssoro E, Dubin A, Laffaire E, et al. Incidence, clinical course, and outcome in 217 patients with acute respiratory distress syndrome. Crit Care Med. 2002;30:2450–2456. - PubMed
-
- Hudson LD, Milberg JA, Anardi D, Maunder RJ. Clinical risks for development of the acute respiratory distress syndrome. Am J Respir Crit Care Med. 1995;151:293–301. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
