

Metabolic support of the obese intensive care unit patient: a current perspective
- PMID: 20040861
- PMCID: PMC3278904
- DOI: 10.1097/MCO.0b013e328335f1e6
Metabolic support of the obese intensive care unit patient: a current perspective
Abstract
Purpose of review: Obesity is a widespread condition associated with a variety of mechanical, metabolic, and physiologic changes that affect both health outcomes and delivery of care. Nutrition support is a key element of management during critical illness known to improve outcomes favorably, but is likewise complicated in the presence of obesity. This review serves to discuss the challenges unique to management of critically ill obese patients and an evidence-based approach to nutrition support in this patient population.
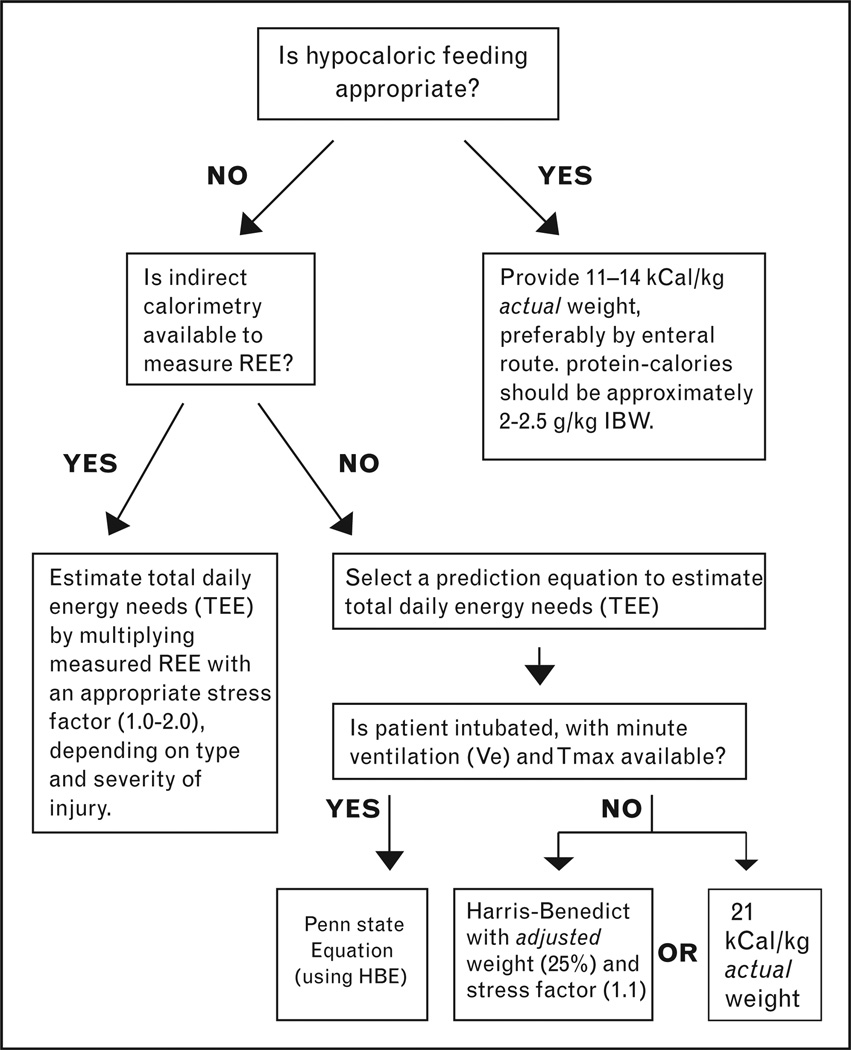
Recent findings: High-protein, hypocaloric feeding has emerged as a nutrition support strategy capable of reducing hyperglycemia and protein catabolism, while promoting favorable changes in body composition and fluid mobilization. Recent data have shown a protective effect of mild-moderate obesity (BMI 30-39.9 kg/m2), with improved morbidity and mortality outcomes in this subgroup. Therefore, it is unclear whether hypocaloric feeding represents an inferior approach in this subgroup in which weight maintenance may be preferable.
Summary: There are many obstacles that limit provision of nutrition support in the obese ICU patient. Calculating energy needs accurately is extremely problematic due to a lack of reliable prediction equations and a wide variability in body composition among the obese patients. Further research is needed to determine a better approach to estimating energy needs in this population, in addition to validating hypocaloric feeding as the standard approach to nutrition support in the obese patients.
Conflict of interest statement
The authors have no conflicts to disclose.
Figures
References
-
- Yach D, Suckler D, Brownel K. Epidemiologic and economic consequences of the global epidemics of obesity and diabetes. Nat Med. 2006;12:62–66. - PubMed
-
- Runge CF. Economic consequences of the obese. Diabetes. 2007;56:2668–2672. - PubMed
-
- Must A, Spadano J, Coakley EH, et al. The disease burden associated with overweight and obesity. JAMA. 1999;282:1523–1529. - PubMed
-
- Calle EE, Rodriguez C, Walker-Thurmond K, Thun MJ. Overweight, obesity, and mortality from cancer in a prospectively studied cohort of U.S. adults. N Engl J Med. 2003;348:1625–1638. - PubMed
-
- Friedenberg FK, Xanthopoulos M, Foster GD, et al. The association between gastroesophageal reflux disease and obesity. Am J Gastroenterol. 2008;103:2111. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
