

Denial of risk behavior does not exclude asymptomatic anorectal sexually transmitted infection in HIV-infected men
- PMID: 20041143
- PMCID: PMC2794382
- DOI: 10.1371/journal.pone.0008504
Denial of risk behavior does not exclude asymptomatic anorectal sexually transmitted infection in HIV-infected men
Abstract
Background: The Centers for Disease Control recommend screening for asymptomatic sexually transmitted infection (STI) among HIV-infected men when there is self-report of unprotected anal-receptive exposure. The study goals were: (1) to estimate the validity and usefulness for screening policies of self-reported unprotected anal-receptive exposure as a risk indicator for asymptomatic anorectal infection with Neisseria gonorrhoeae (GC) and/or Chlamydia trachomatis (CT). (2) to estimate the number of infections that would be missed if anal diagnostic assays were not performed among patients who denied unprotected anorectal exposure in the preceding month.
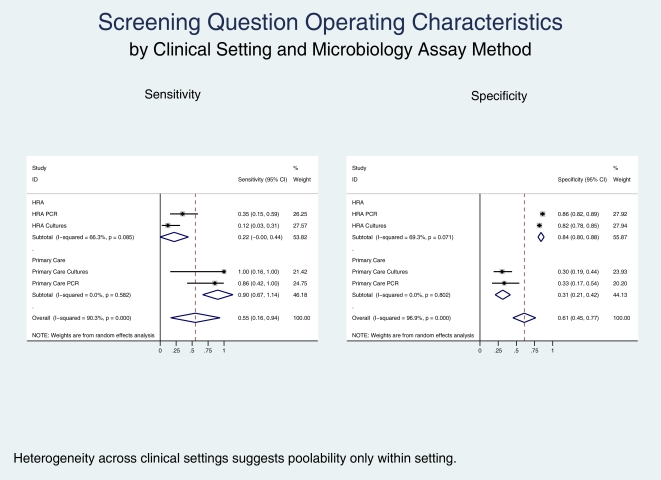
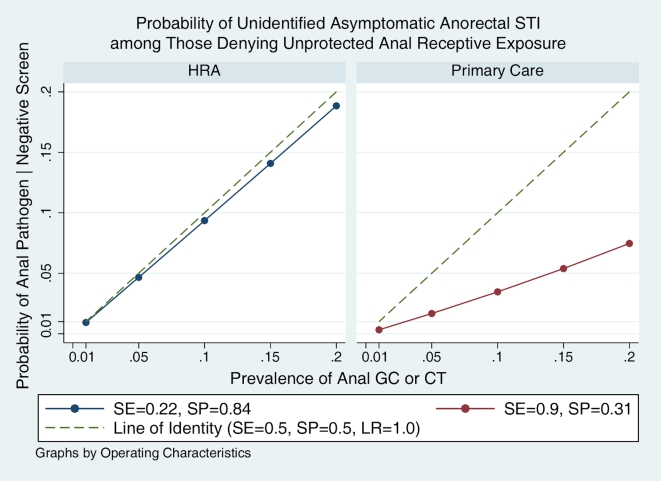
Methods and findings: Retrospective analysis in HIV primary care and high resolution anoscopy (HRA) clinics. HIV-infected adult men were screened for self-reported exposure during the previous month at all primary care and HRA appointments. Four sub-cohorts were defined based on microbiology methodology (GC culture and CT direct fluorescent antibody vs. GC/CT nucleic acid amplification test) and clinical setting (primary care vs. HRA). Screening question operating characteristics were estimated using contingency table methods and then pooled across subcohorts. Among 803 patients, the prevalence of anorectal GC/CT varied from 3.5-20.1% in the 4 sub-cohorts. The sensitivity of the screening question for self-reported exposure to predict anorectal STI was higher in the primary care than in the HRA clinic, 86-100% vs. 12-35%, respectively. The negative predictive value of the screening question to predict asymptomatic anorectal STI was > or = 90% in all sub-cohorts. In sensitivity analyses, the probability of being an unidentified case among those denying exposure increased from 0.4-8.1% in the primary care setting, and from 0.9-18.8% in the HRA setting as the prevalence varied from 1-20%.
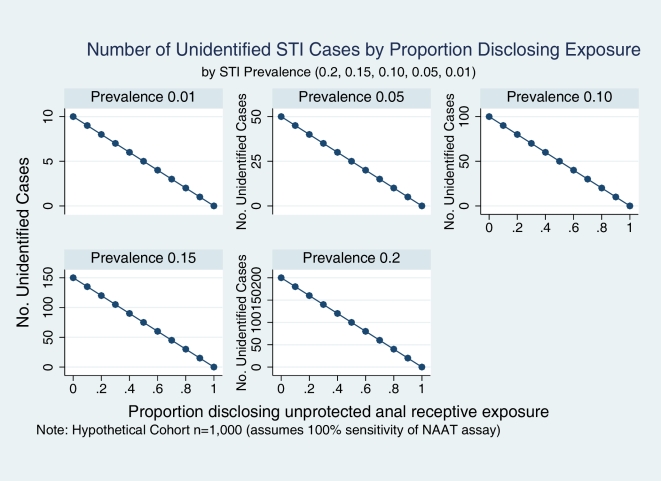
Conclusion: As STI prevalence increases, denial of unprotected anal-receptive exposure leads to an increasingly unacceptable proportion of unidentified asymptomatic anorectal STI if used as a criterion not to obtain microbiologic assays.
Conflict of interest statement
Figures
References
-
- Workowski KA, Berman SM. Sexually transmitted diseases treatment guidelines, 2006. MMWR Recomm Rep. 2006;55:1–94. - PubMed
-
- Aberg JA, Kaplan JE, Libman H, Emmanuel P, Anderson JR, et al. Primary care guidelines for the management of persons infected with human immunodeficiency virus: 2009 update by the HIV Medicine Association of the Infectious Diseases Society of America. Clin Infect Dis. 2009;49:651–681. - PubMed
-
- Hoover K. Sexually transmitted disease testing of HIV-infected men who have sex with men at eight U.S. Clinics [Poster 143]. 2008 National STD prevention conference, Chicago, Ill. March 10–13. 2008. Available: http://www.cdc.gov/stdconference/2008/press/summaries-12march2008.htm. Accessed 2009 Jul 15.
-
- Cachay E, Mar-Tang M, Mathews WC. Screening for potentially transmitting sexual risk behaviors, urethral sexually transmitted infection, and sildenafil use among males entering care for HIV infection. AIDS Patient Care STDS. 2004;18:349–354. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
