

Abdominal compression increases upper airway collapsibility during sleep in obese male obstructive sleep apnea patients
- PMID: 20041593
- PMCID: PMC2786041
- DOI: 10.1093/sleep/32.12.1579
Abdominal compression increases upper airway collapsibility during sleep in obese male obstructive sleep apnea patients
Abstract
Study objectives: Abdominal obesity, particularly common in centrally obese males, may have a negative impact on upper airway (UA) function during sleep. For example, cranial displacement of the diaphragm with raised intra-abdominal pressure may reduce axial tension exerted on the UA by intrathoracic structures and increase UA collapsibility during sleep.
Design: This study aimed to examine the effect of abdominal compression on UA function during sleep in obese male obstructive sleep apnea patients.
Setting: Participants slept in a sound-insulated room with physiologic measurements controlled from an adjacent room.
Participants: Fifteen obese (body mass index: 34.5 +/- 1.1 kg/m2) male obstructive sleep apnea patients (apnea-hypopnea index: 58.1 +/- 6.8 events/h) aged 50 +/- 2.6 years participated.
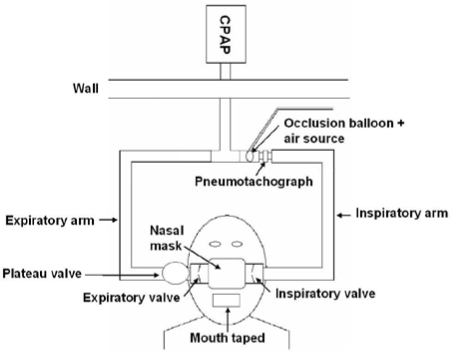
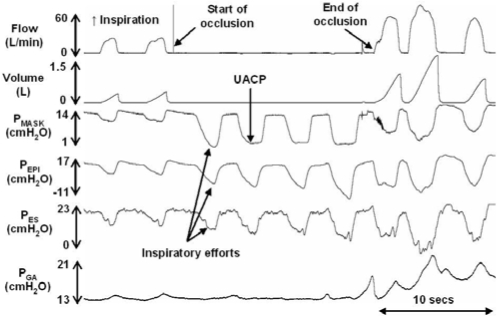
Interventions: Gastric (PGA) and transdiaphragmatic pressures (P(DI)), UA closing pressure (UACP), UA airflow resistance (R(UA)), and changes in end-expiratory lung volume (EELV) were determined during stable stage 2 sleep with and without abdominal compression, achieved via inflation of a pneumatic cuff placed around the abdomen. UACP was assessed during brief mask occlusions.
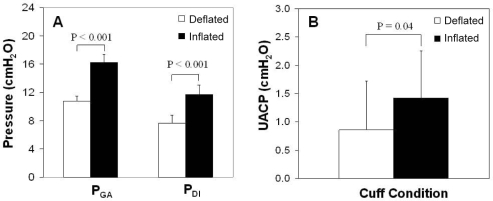
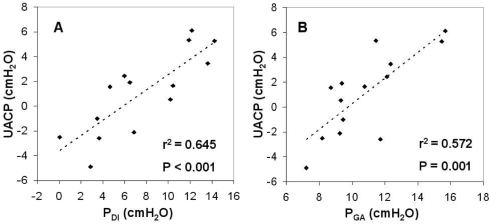
Measurements and results: Abdominal compression significantly decreased EELV by 0.53 +/- 0.24 L (P=0.045) and increased PGA (16.2 +/- 0.8 versus 10.8 +/- 0.7 cm H2O, P < 0.001), P(DI) (11.7 +/- 0.9 versus 7.6 +/- 1.2 cm H2O, P < 0.001) and UACP (1.4 +/- 0.8 versus 0.9 +/- 0.9 cm H2O, P = 0.039) but not R(UA)(6.5 +/- 1.4 versus 6.9 +/- 1.4 cm H2O x L/s, P=0.585).
Conclusions: Abdominal compression negatively impacts on UA collapsibility during sleep and this effect may help explain strong associations between central obesity and obstructive sleep apnea.
Figures
Similar articles
-
Effects of Altered Intra-abdominal Pressure on the Upper Airway Collapsibility in a Porcine Model.Chin Med J (Engl). 2015 Dec 5;128(23):3204-10. doi: 10.4103/0366-6999.170281. Chin Med J (Engl). 2015. PMID: 26612297 Free PMC article.
-
Dynamic modulation of upper airway function during sleep: a novel single-breath method.J Appl Physiol (1985). 2006 Nov;101(5):1489-94. doi: 10.1152/japplphysiol.00173.2006. Epub 2006 Jul 6. J Appl Physiol (1985). 2006. PMID: 16825526
-
Negative Expiratory Pressure Technique: An Awake Test to Measure Upper Airway Collapsibility in Adolescents.Sleep. 2015 Nov 1;38(11):1783-91. doi: 10.5665/sleep.5164. Sleep. 2015. PMID: 26158888 Free PMC article. Clinical Trial.
-
Obesity and upper airway control during sleep.J Appl Physiol (1985). 2010 Feb;108(2):430-5. doi: 10.1152/japplphysiol.00919.2009. Epub 2009 Oct 29. J Appl Physiol (1985). 2010. PMID: 19875707 Free PMC article. Review.
-
Obesity and obstructive sleep apnea: pathogenic mechanisms and therapeutic approaches.Proc Am Thorac Soc. 2008 Feb 15;5(2):185-92. doi: 10.1513/pats.200708-137MG. Proc Am Thorac Soc. 2008. PMID: 18250211 Free PMC article. Review.
Cited by
-
Defining phenotypic causes of obstructive sleep apnea. Identification of novel therapeutic targets.Am J Respir Crit Care Med. 2013 Oct 15;188(8):996-1004. doi: 10.1164/rccm.201303-0448OC. Am J Respir Crit Care Med. 2013. PMID: 23721582 Free PMC article.
-
Effects of Altered Intra-abdominal Pressure on the Upper Airway Collapsibility in a Porcine Model.Chin Med J (Engl). 2015 Dec 5;128(23):3204-10. doi: 10.4103/0366-6999.170281. Chin Med J (Engl). 2015. PMID: 26612297 Free PMC article.
-
Control of the pharyngeal musculature during wakefulness and sleep: implications in normal controls and sleep apnea.Head Neck. 2011 Oct;33 Suppl 1(Suppl 1):S37-45. doi: 10.1002/hed.21841. Epub 2011 Sep 7. Head Neck. 2011. PMID: 21901775 Free PMC article. Review.
-
Treatment of Obstructive Sleep Apnea. Prospects for Personalized Combined Modality Therapy.Ann Am Thorac Soc. 2016 Jan;13(1):101-8. doi: 10.1513/AnnalsATS.201508-537FR. Ann Am Thorac Soc. 2016. PMID: 26569377 Free PMC article. Review.
-
Should visceral fat, strictly linked to hepatic steatosis, be depleted to improve survival?Hepatol Int. 2013 Jun;7(2):413-28. doi: 10.1007/s12072-012-9406-z. Epub 2012 Oct 26. Hepatol Int. 2013. PMID: 26201775
References
-
- Dixon JB, Schachter LM, O'Brien PE. Predicting sleep apnea and excessive day sleepiness in the severely obese. Chest. 2003;123:1134–41. - PubMed
-
- Young T, Palta M, Dempsey J, Skatrud J, Weber S, Badr S. The occurrence of sleep-disordered breathing among middle-aged adults. N Engl J Med. 1993;328:1230–5. - PubMed
-
- Rowley JA, Permutt S, Willey S, Smith PL, Schwartz AR. Effect of tracheal and tongue displacement on upper airway airflow dynamics. J Appl Physiol. 1996;80:2171–8. - PubMed
-
- Van de Graaff WB. Thoracic influence on upper airway patency. J Appl Physiol. 1988;65:2124–31. - PubMed
-
- Series F, Marc I. Influence of lung volume dependence of upper airway resistance during continuous negative airway pressure. J Appl Physiol. 1994;77:840–4. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
