

Sedation depth during spinal anesthesia and the development of postoperative delirium in elderly patients undergoing hip fracture repair
- PMID: 20042557
- PMCID: PMC2800291
- DOI: 10.4065/mcp.2009.0469
Sedation depth during spinal anesthesia and the development of postoperative delirium in elderly patients undergoing hip fracture repair
Erratum in
- Mayo Clin Proc. 2010 Apr;85(4):400. Dosage error in article text
Abstract
Objective: To determine whether limiting intraoperative sedation depth during spinal anesthesia for hip fracture repair in elderly patients can decrease the prevalence of postoperative delirium.
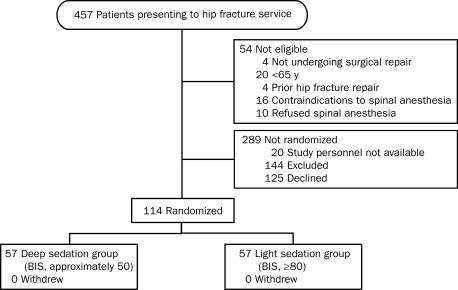
Patients and methods: We performed a double-blind, randomized controlled trial at an academic medical center of elderly patients (>or=65 years) without preoperative delirium or severe dementia who underwent hip fracture repair under spinal anesthesia with propofol sedation. Sedation depth was titrated using processed electroencephalography with the bispectral index (BIS), and patients were randomized to receive either deep (BIS, approximately 50) or light (BIS, >or=80) sedation. Postoperative delirium was assessed as defined by Diagnostic and Statistical Manual of Mental Disorders (Third Edition Revised) criteria using the Confusion Assessment Method beginning at any time from the second day after surgery.
Results: From April 2, 2005, through October 30, 2008, a total of 114 patients were randomized. The prevalence of postoperative delirium was significantly lower in the light sedation group (11/57 [19%] vs 23/57 [40%] in the deep sedation group; P=.02), indicating that 1 incident of delirium will be prevented for every 4.7 patients treated with light sedation. The mean +/- SD number of days of delirium during hospitalization was lower in the light sedation group than in the deep sedation group (0.5+/-1.5 days vs 1.4+/-4.0 days; P=.01).
Conclusion: The use of light propofol sedation decreased the prevalence of postoperative delirium by 50% compared with deep sedation. Limiting depth of sedation during spinal anesthesia is a simple, safe, and cost-effective intervention for preventing postoperative delirium in elderly patients that could be widely and readily adopted.
Trial registration: ClinicalTrials.gov NCT00590707.
Figures
Comment in
-
Delirium: a cognitive cost of the comfort of procedural sedation in elderly patients?Mayo Clin Proc. 2010 Jan;85(1):12-4. doi: 10.4065/mcp.2009.0724. Mayo Clin Proc. 2010. PMID: 20042555 Free PMC article. No abstract available.
References
-
- Rasmussen LS, Moller JT. Central nervous system dysfunction after anesthesia in the geriatric patient. Anesthesiol Clin North America 2000;18(1):59-70, vi - PubMed
-
- Dyer CB, Ashton CM, Teasdale TA. Postoperative delirium: a review of 80 primary data-collection studies. Arch Intern Med. 1995;155(5):461-465 - PubMed
-
- Bitsch MS, Foss NB, Kristensen BB, Kehlet H. Acute cognitive dysfunction after hip fracture: frequency and risk factors in an optimized, multimodal, rehabilitation program. Acta Anaesthesiol Scand. 2006;50(4):428-436 - PubMed
-
- Sharma PT, Sieber FE, Zakriya KJ, et al. Recovery room delirium predicts postoperative delirium after hip-fracture repair. Anesth Analg. 2005;101(4):1215-1220 - PubMed
-
- Zakriya K, Sieber FE, Christmas C, Wenz JF, Sr, Franckowiak S. Brief postoperative delirium in hip fracture patients affects functional outcome at three months. Anesth Analg. 2004;98(6):1798-1802 - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
